

Performance of closed-loop resuscitation of haemorrhagic shock with fluid alone or in combination with norepinephrine: an experimental study
- PMID: 30225814
- PMCID: PMC6141407
- DOI: 10.1186/s13613-018-0436-0
Performance of closed-loop resuscitation of haemorrhagic shock with fluid alone or in combination with norepinephrine: an experimental study
Abstract
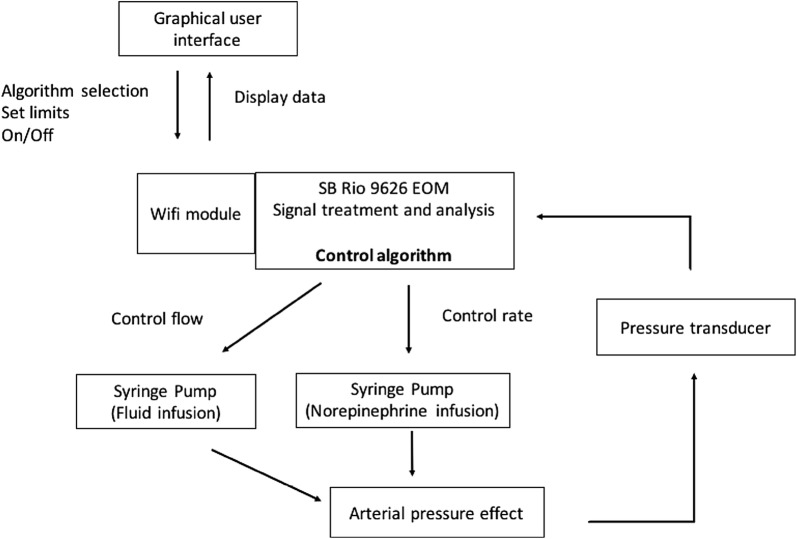
Background: Closed-loop resuscitation can improve personalization of care, decrease workload and bring expert knowledge in isolated areas. We have developed a new device to control the administration of fluid or simultaneous co-administration of fluid and norepinephrine using arterial pressure.
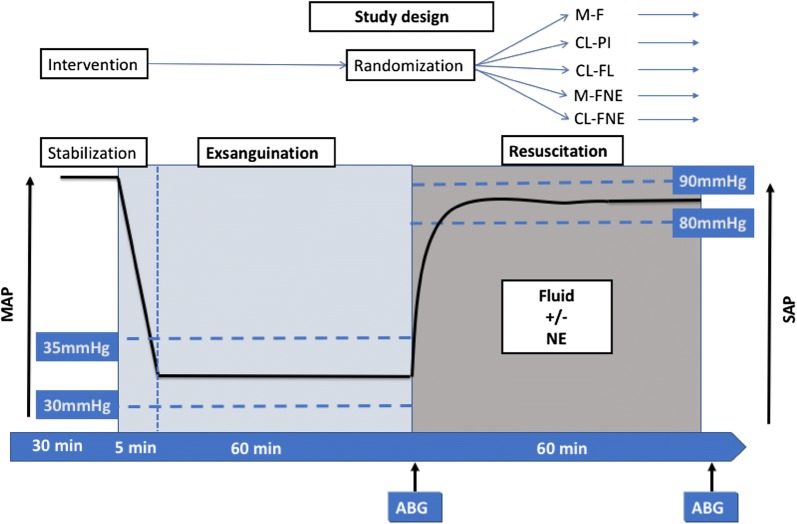
Method: We evaluated the performance of our prototype in a rodent model of haemorrhagic shock. After haemorrhagic shock, rats were randomized to five experimental groups: three were resuscitated with fluid and two with co-administration of fluid and norepinephrine. Among groups resuscitated with fluid, one was resuscitated by a physician and two were resuscitated according to two different closed-loop algorithms. Among groups resuscitated with fluid and norepinephrine, one was resuscitated by a physician and the other one by the closed-loop device. The precision of arterial pressure during the resuscitation period was assessed using rising time, time passed in the target area and performance error calculations.
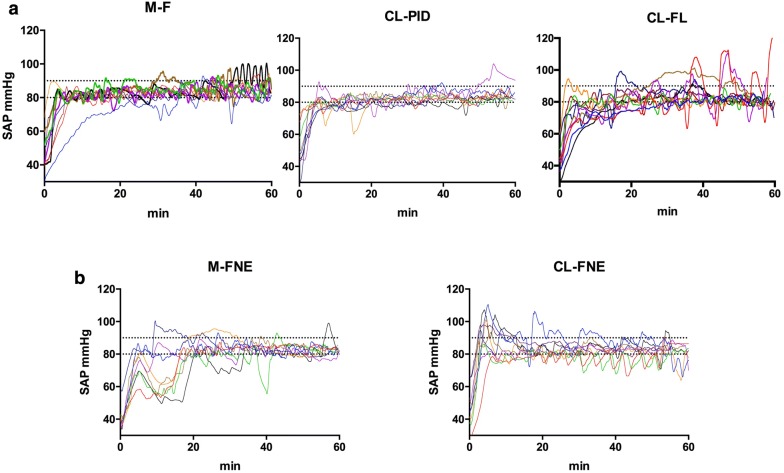
Results: Groups resuscitated with fluid had similar performances and passed as much time in the target area of 80-90 mmHg as the manual group [manual: 76.8% (67.9-78.2), closed-loop: 64.6% (45.7-72.9) and 80.9% (59.1-85.3)]. Rats resuscitated with fluid and norepinephrine using closed-loop passed similar time in target area than manual group [closed-loop: 74.4% (58.4-84.5) vs. manual: 60.1% (46.1-72.4)] but had shorter rising time to reach target area [160 s (106-187) vs. 434 s (254-1081)] than those resuscitated by a physician. Rats resuscitated with co-administration of fluid and norepinephrine required less fluid and had less hemodilution than rats resuscitated with fluid alone. Lactate decrease was similar between groups resuscitated with fluid alone and fluid with norepinephrine.
Conclusions: This study assessed extensively the performances of several algorithms for closed-loop resuscitation of haemorrhagic shock with fluid alone and with co-administration of fluid and norepinephrine. The performance of the closed-loop algorithms tested was similar to physician-guided treatment with considerable saving of work for the caregiver. Arterial pressure closed-loop guided algorithms can be extended to combined administration of fluid and norepinephrine.
Keywords: Closed-loop; Fluid; Haemorrhagic shock; Norepinephrine; Resuscitation.
Figures
Similar articles
-
Closed-Loop Control for Fluid Resuscitation: Recent Advances and Future Challenges.Front Vet Sci. 2021 Feb 23;8:642440. doi: 10.3389/fvets.2021.642440. eCollection 2021. Front Vet Sci. 2021. PMID: 33708814 Free PMC article. Review.
-
Performance of closed-loop resuscitation in a pig model of haemorrhagic shock with fluid alone or in combination with norepinephrine, a pilot study.J Clin Monit Comput. 2021 Aug;35(4):835-847. doi: 10.1007/s10877-020-00542-7. Epub 2020 Jun 12. J Clin Monit Comput. 2021. PMID: 32533529
-
Renal Microcirculation and Function in a Pig Model of Hemorrhagic Shock Resuscitation with Norepinephrine.Am J Respir Crit Care Med. 2022 Jul 1;206(1):34-43. doi: 10.1164/rccm.202109-2120OC. Am J Respir Crit Care Med. 2022. PMID: 35394403
-
Comparative effects of early versus delayed use of norepinephrine in resuscitated endotoxic shock.Crit Care Med. 2007 Jul;35(7):1736-40. doi: 10.1097/01.CCM.0000269028.28521.08. Crit Care Med. 2007. PMID: 17522580
-
Closed-Loop Controlled Fluid Administration Systems: A Comprehensive Scoping Review.J Pers Med. 2022 Jul 18;12(7):1168. doi: 10.3390/jpm12071168. J Pers Med. 2022. PMID: 35887665 Free PMC article.
Cited by
-
Closed-Loop Control for Fluid Resuscitation: Recent Advances and Future Challenges.Front Vet Sci. 2021 Feb 23;8:642440. doi: 10.3389/fvets.2021.642440. eCollection 2021. Front Vet Sci. 2021. PMID: 33708814 Free PMC article. Review.
-
Automated closed-loop versus manually controlled norepinephrine infusion in patients undergoing intermediate- to high-risk abdominal surgery: a randomised controlled trial.Br J Anaesth. 2021 Jan;126(1):210-218. doi: 10.1016/j.bja.2020.08.051. Epub 2020 Oct 8. Br J Anaesth. 2021. PMID: 33041014 Free PMC article. Clinical Trial.
-
Evaluating an advanced double intravenous vasopressor automated system to treat hypotension during spinal anesthesia for cesarean delivery: a randomized controlled trial.BMC Anesthesiol. 2023 Jan 26;23(1):33. doi: 10.1186/s12871-023-01992-7. BMC Anesthesiol. 2023. PMID: 36703120 Free PMC article. Clinical Trial.
-
Feasibility of closed-loop titration of norepinephrine infusion in patients undergoing moderate- and high-risk surgery.Br J Anaesth. 2019 Oct;123(4):430-438. doi: 10.1016/j.bja.2019.04.064. Epub 2019 Jun 27. Br J Anaesth. 2019. PMID: 31255290 Free PMC article.
-
Computer-controlled closed-loop norepinephrine infusion system for automated control of mean arterial pressure in dogs under isoflurane-induced hypotension: a feasibility study.Front Vet Sci. 2024 May 31;11:1374356. doi: 10.3389/fvets.2024.1374356. eCollection 2024. Front Vet Sci. 2024. PMID: 38881786 Free PMC article.
References
-
- Sondeen JL, Coppes VG, Holcomb JB. Blood pressure at which rebleeding occurs after resuscitation in swine with aortic injury. J Trauma. 2003;54(5 Suppl):S110–S117. - PubMed
-
- Burgert JM, Gegel BT, Austin R, 3rd, Davila A, Deeds J, Hodges L, et al. Effects of arterial blood pressure on rebleeding using Celox and TraumaDEX in a porcine model of lethal femoral injury. AANA J. 2010;78(3):230–236. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
