

Candida auris in Healthcare Facilities, New York, USA, 2013-2017
- PMID: 30226155
- PMCID: PMC6154128
- DOI: 10.3201/eid2410.180649
Candida auris in Healthcare Facilities, New York, USA, 2013-2017
Abstract
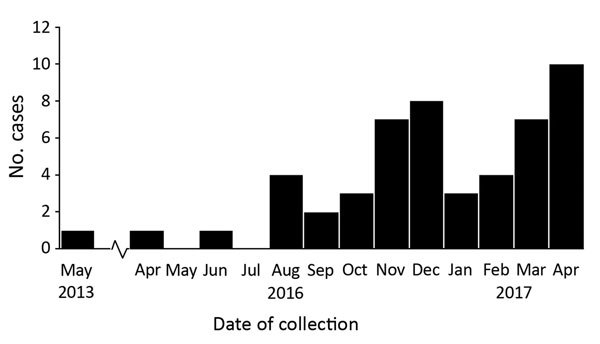
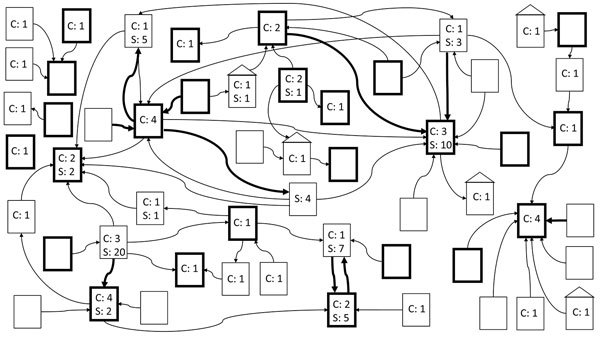
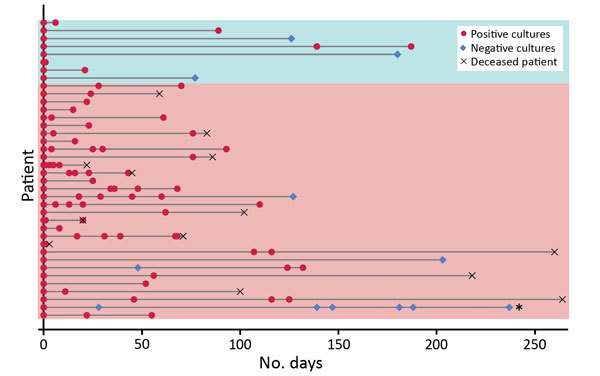
Candida auris is an emerging yeast that causes healthcare-associated infections. It can be misidentified by laboratories and often is resistant to antifungal medications. We describe an outbreak of C. auris infections in healthcare facilities in New York City, New York, USA. The investigation included laboratory surveillance, record reviews, site visits, contact tracing with cultures, and environmental sampling. We identified 51 clinical case-patients and 61 screening case-patients. Epidemiologic links indicated a large, interconnected web of affected healthcare facilities throughout New York City. Of the 51 clinical case-patients, 23 (45%) died within 90 days and isolates were resistant to fluconazole for 50 (98%). Of screening cultures performed for 572 persons (1,136 total cultures), results were C. auris positive for 61 (11%) persons. Environmental cultures were positive for samples from 15 of 20 facilities. Colonization was frequently identified during contact investigations; environmental contamination was also common.
Keywords: Candida auris; New York; United States; epidemiology; fungi; healthcare facilities; infection control; yeast.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
