

Landscape of EGFR-Dependent and -Independent Resistance Mechanisms to Osimertinib and Continuation Therapy Beyond Progression in EGFR-Mutant NSCLC
- PMID: 30228210
- PMCID: PMC6295279
- DOI: 10.1158/1078-0432.CCR-18-1542
Landscape of EGFR-Dependent and -Independent Resistance Mechanisms to Osimertinib and Continuation Therapy Beyond Progression in EGFR-Mutant NSCLC
Abstract
Purpose: Osimertinib was initially approved for T790M-positive non-small cell lung cancer (NSCLC) and, more recently, for first-line treatment of EGFR-mutant NSCLC. However, resistance mechanisms to osimertinib have been incompletely described.
Experimental design: Using cohorts from The University of Texas MD Anderson Lung Cancer Moonshot GEMINI and Moffitt Cancer Center lung cancer databases, we collected clinical data for patients treated with osimertinib. Molecular profiling analysis was performed at the time of progression in a subset of the patients.
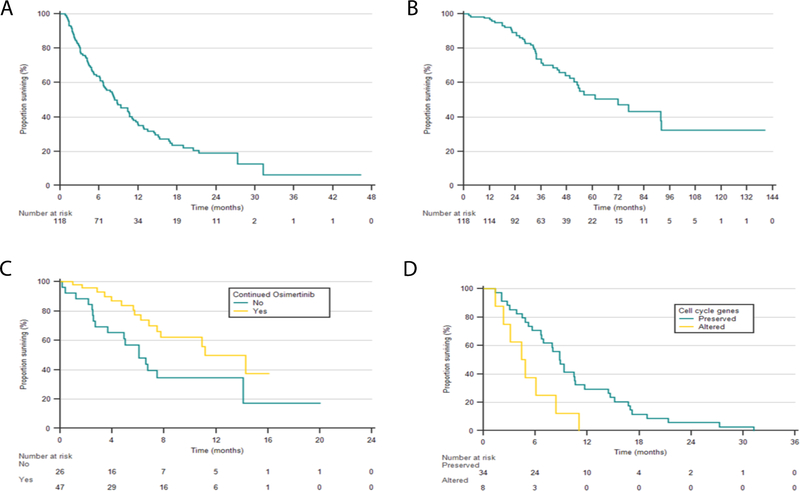
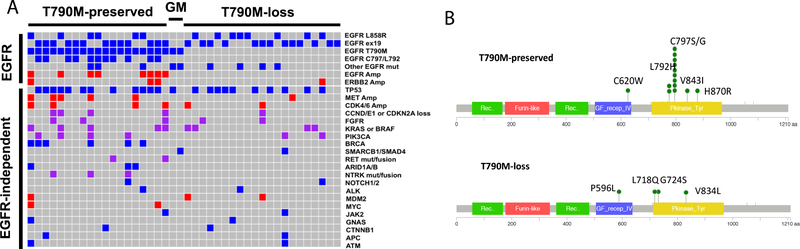
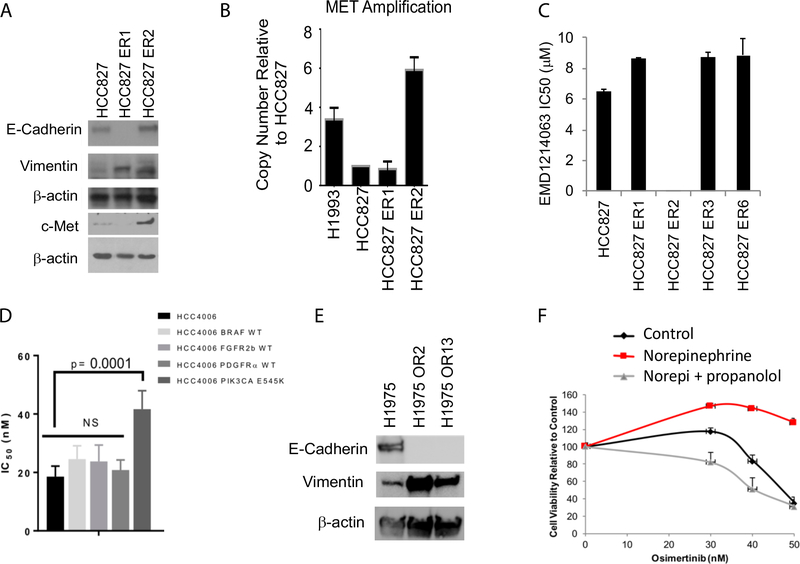
Results: In the 118 patients treated with osimertinib, 42 had molecular profiling at progression. T790M was preserved in 21 (50%) patients and lost in 21 (50%). EGFR C797 and L792 (26%) mutations were the most common resistance mechanism and were observed exclusively in T790M-preserved cases. MET amplification was the second most common alteration (14%). Recurrent alterations were observed in 22 genes/pathways, including PIK3CA, FGFR, and RET. Preclinical studies confirmed MET, PIK3CA, and epithelial-to-mesenchymal transition as potential resistance drivers. Alterations of cell-cycle genes were associated with shorter median progression-free survival (PFS, 4.4 vs. 8.8 months, P = 0.01). In 76 patients with progression, osimertinib was continued in 47 cases with a median second PFS (PFS2) of 12.6 months; 21 patients received local consolidation radiation with a median PFS of 15.5 months. Continuation of osimertinib beyond progression was associated with a longer overall survival compared with discontinuation (11.2 vs. 6.1 months, P = 0.02).
Conclusions: Osimertinib resistance is associated with diverse, predominantly EGFR-independent genomic alterations. Continuation of osimertinib after progression, alone or in conjunction with radiotherapy, may provide prolonged clinical benefit in selected patients.See related commentary by Devarakonda and Govindan, p. 6112.
©2018 American Association for Cancer Research.
Conflict of interest statement
Conflict of interest: Dr. Le received a consultant fee from Eli Lilly AstraZeneca and Boehringer Ingelheim. Dr. Papadimitrakopoulou receives a consultant fee from AstraZeneca. Dr. Gray is an advisor for AstraZeneca, Boehringer Ingelheim and Genentech. Dr. Heymach is an advisor for AstraZeneca, Boehringer Ingelheim, EMD Serono, Genentech, Eli Lily, Merck, Roche, Spectrum, Guardant, Janssen, Novartis, Foundation Medicine. Other authors do not report relevant conflict of interest.
Figures
Comment in
-
Targeting Resistance to Targeted Therapies: Combating a Resilient Foe.Clin Cancer Res. 2018 Dec 15;24(24):6112-6114. doi: 10.1158/1078-0432.CCR-18-3178. Epub 2018 Oct 23. Clin Cancer Res. 2018. PMID: 30352903 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
