

The Microbiome and Tuberculosis: Early Evidence for Cross Talk
- PMID: 30228238
- PMCID: PMC6143735
- DOI: 10.1128/mBio.01420-18
The Microbiome and Tuberculosis: Early Evidence for Cross Talk
Abstract
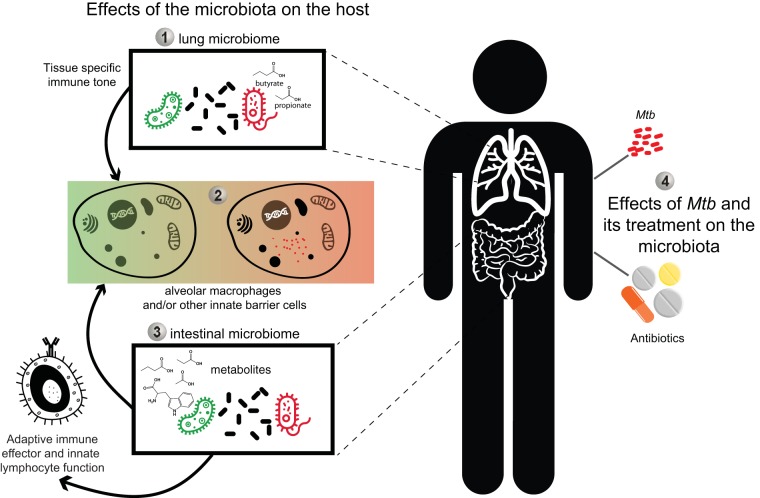
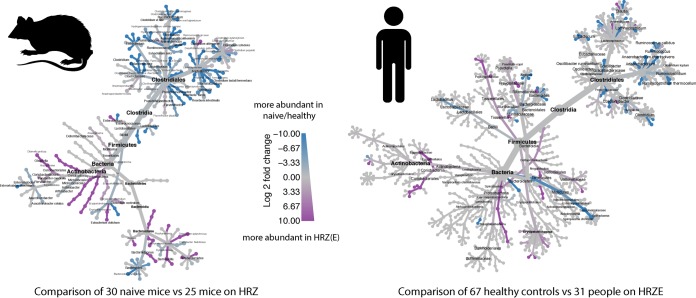
Tuberculosis (TB) is an ancient infectious disease of humans that has been extensively studied both clinically and experimentally. Although susceptibility to Mycobacterium tuberculosis infection is clearly influenced by factors such as nutrition, immune status, and both mycobacterial and host genetics, the variable pathogenesis of TB in infected individuals remains poorly understood. During the past two decades, it has become clear that the microbiota-the trillion organisms that reside at mucosal surfaces within and on the body-can exert a major influence on disease outcome through its effects on host innate and adaptive immune function and metabolism. This new recognition of the potentially pleiotropic participation of the microbiome in immune responses has raised the possibility that the microbiota may influence M. tuberculosis infection and/or disease. Similarly, treatment of TB may alter the healthy steady-state composition and function of the microbiome, possibly affecting treatment outcome in addition to other host physiological parameters. Herein, we review emerging evidence for how the microbiota may influence the transition points in the life cycle of TB infection, including (i) resistance to initial infection, (ii) initial infection to latent tuberculosis (LTBI), (iii) LTBI to reactivated disease, and (iv) treatment to cure. A major goal of this review is to frame questions to guide future scientific and clinical studies in this largely unexplored but increasingly important area of TB research.
Keywords: antibiotics; microbiome; tuberculosis.
Figures
References
-
- WHO. 2016. Global tuberculosis report. WHO, Geneva, Switzerland.
-
- Cobat A, Gallant CJ, Simkin L, Black GF, Stanley K, Hughes J, Doherty TM, Hanekom WA, Eley B, Jaïs J-P, Boland-Auge A, van Helden P, Casanova J-L, Abel L, Hoal EG, Schurr E, Alcaïs A. 2009. Two loci control tuberculin skin test reactivity in an area hyperendemic for tuberculosis. J Exp Med 206:2583–2591. doi:10.1084/jem.20090892. - DOI - PMC - PubMed
-
- Anonymous 1981. Controlled clinical trial of five short-course (4-month) chemotherapy regimens in pulmonary tuberculosis. Second report of the 4th study. East African/British Medical Research Councils Study. Am Rev Respir Dis 123:165–170. - PubMed
-
- Anonymous 1979. Sputum-smear-negative pulmonary tuberculosis: controlled trial of 3-month and 2-month regimens of chemotherapy. Lancet i:1361–1363. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
