

The clinical importance of a cytokine network in the acute phase of sepsis
- PMID: 30228372
- PMCID: PMC6143513
- DOI: 10.1038/s41598-018-32275-8
The clinical importance of a cytokine network in the acute phase of sepsis
Abstract
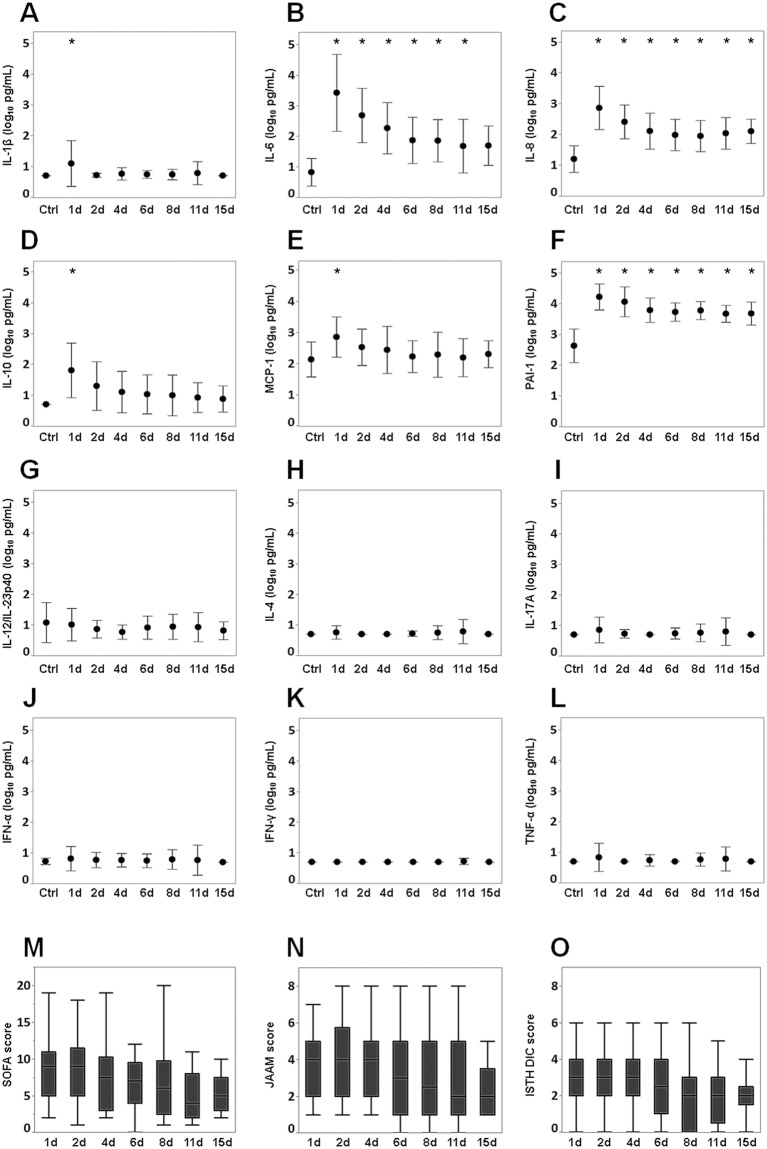
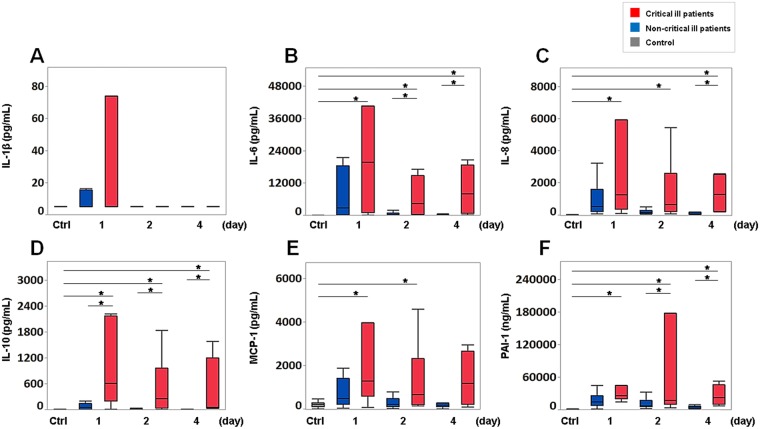
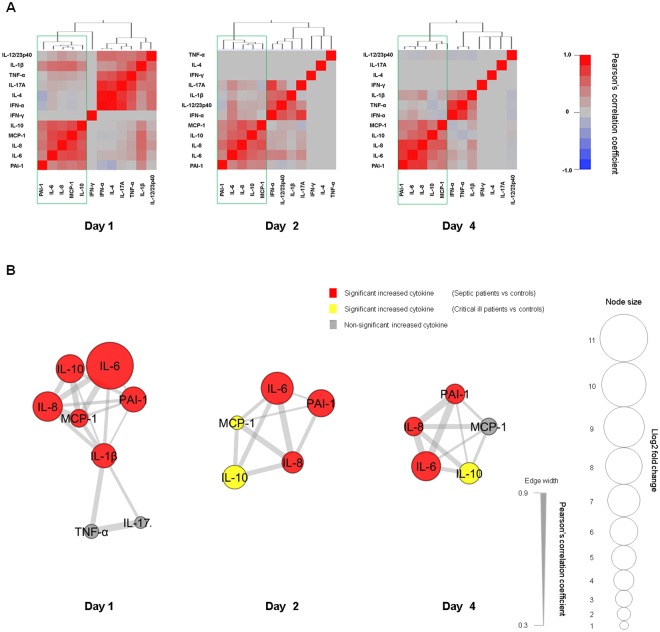
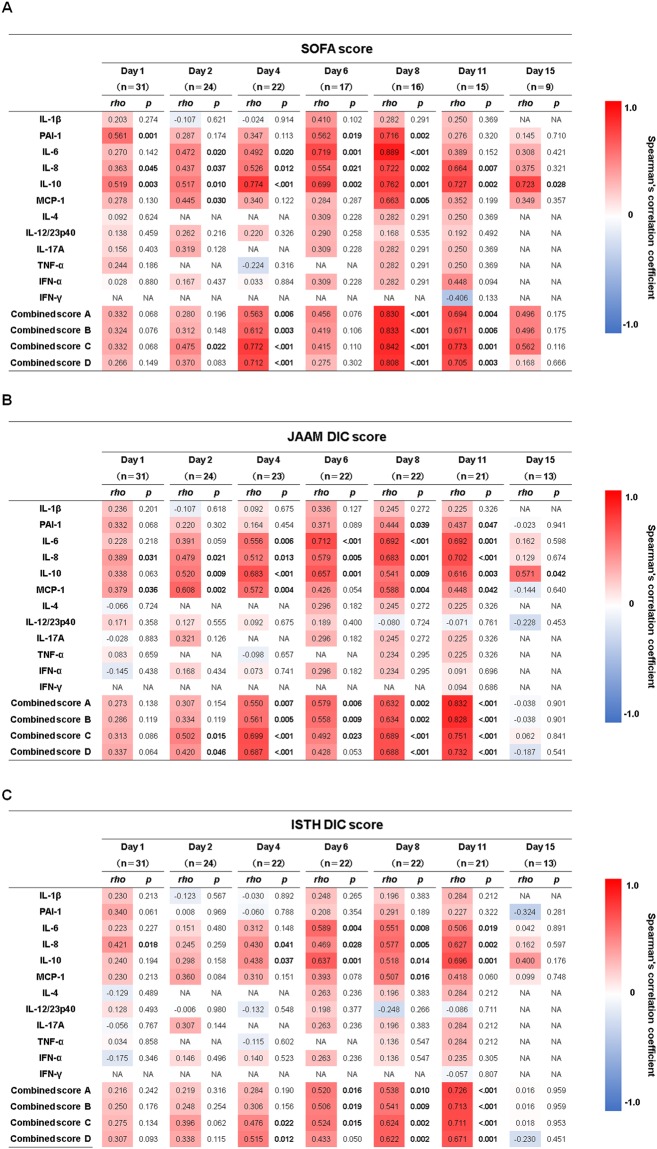
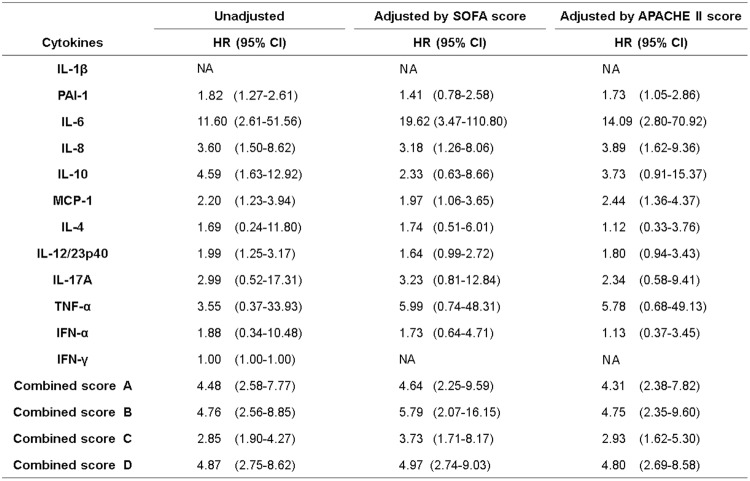
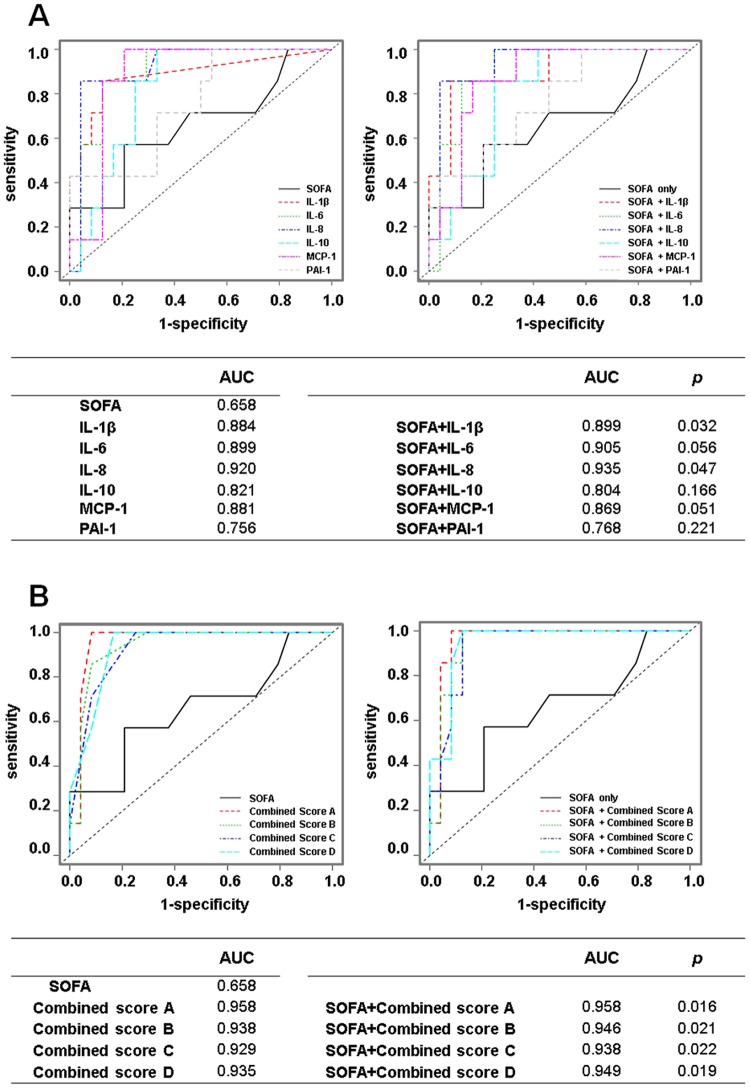
Sepsis remains a major cause of death. Cytokines interact closely with each other and play a crucial role in the progression of sepsis. We focussed on the associations of a cytokine network with prognosis and disease severities in sepsis. This retrospective study included 31 patients with sepsis and 13 healthy controls. Blood samples were collected from patients on days 1, 2, 4, 6, 8, 11 and 15 and from healthy controls. Levels of PAI-1, IFN-α, IFN-γ, IL-1β, IL-6, IL-8, IL-12/IL-23p40, IL-17A, TNF-α, MCP-1, IL-4 and IL-10 were measured. SOFA, JAAM DIC and ISTH DIC scores were evaluated at the same times blood samples were taken. Network analysis revealed a network formed by PAI-1, IL-6, IL-8, MCP-1 and IL-10 on days 1, 2 and 4 throughout the acute phase of sepsis. There were positive correlations of each cytokine and the combined score (IL-6 + IL-8 + IL-10 + MCP-1) with the SOFA, JAAM DIC and ISTH DIC scores throughout the acute phase. A Cox proportional hazards model focussed on the acute phase showed that the above combined score was significantly related with patient prognosis, suggesting that the cytokine network of IL-6, IL-8, MCP-1 and IL-10 could play a pivotal role in the acute phase of sepsis.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
