

Review
Dysphagia
Mo Med.
2018 May-Jun.
Abstract
A complaint of dysphagia suggests difficulty in swallowing and is characterized based on the symptoms and location of pathology. Oropharyngeal dysphagia is typically due to difficulty initiating a swallow and is generally due to structural, anatomic or neuromuscular abnormalities. Esophageal dysphagia arises after the swallow and causes include intrinsic structural pathology, extrinsic compression, or disruption in normal motility. Etiologies, methods of evaluation, and management options of dysphagia are reviewed here.
Figures
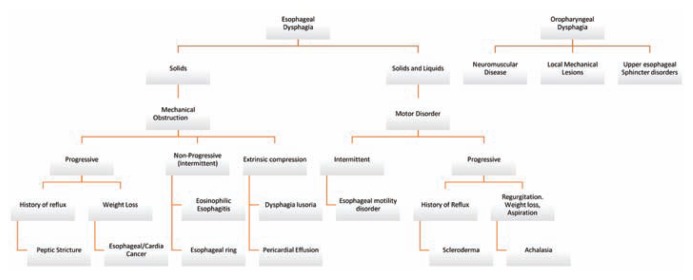
Differential diagnosis of common presentations of dysphagia.
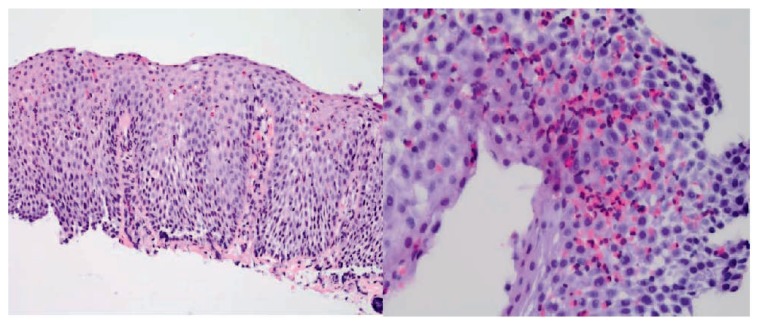
Photomicrograph of an esophageal biopsy obtained during routine upper endoscopy shows squamous mucosa with increased intraepithelial eosinophils, basal hyperplasia, and elongation of papillae. Photo credit: Paul Friedman, MD, Department of Pathology, Saint Louis University School of Medicine.
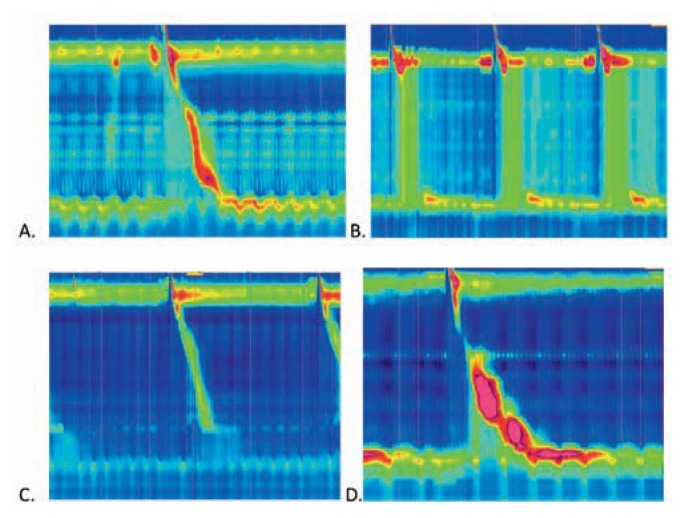
High resolution manometry images demonstrate the pressures along the length of the esophagus (vertical axis) over time (horizonal axis) after swallows in the setting of common abnormalities. A. Normal esophageal manometry with normal progression of the pressure wave over time; B. Manometry in achalasia type II (classic achalasia) shows a lack of a normal peristaltic pressure wave; C. Manometry demonstrating weak lower esophageal sphincter (LES) tone that predisposes to GERD; D. Manometry demonstrating esophagogastric junction outflow obstruction (EGJOO) due to abnormally high pressures. Photo credit: Charlene Prather, MD, Division of Gastroenterology and Hepatology, Saint Louis University School of Medicine.



References
-
- Abdel Jalil AA, Katzka DA, Castell DO. Approach to the patient with dysphagia. Am J Med. 2015;128:1138 e1117–1123. - PubMed
-
- Yamada’s Handbook of Gastroenterology. 3 ed. Wiley-Blackwell; 2013.
-
- Spieker MR. Evaluating dysphagia. Am Fam Physician. 2000;61:3639–3648. - PubMed
-
- Eslick GD, Talley NJ. Dysphagia: epidemiology, risk factors and impact on quality of life--a population-based study. Aliment Pharmacol Ther. 2008;27:971–979. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical