

Boerhaave syndrome in an elderly man successfully treated with 3-month indwelling esophageal stent
- PMID: 30228849
- PMCID: PMC6137399
- DOI: 10.1016/j.radcr.2018.04.026
Boerhaave syndrome in an elderly man successfully treated with 3-month indwelling esophageal stent
Abstract
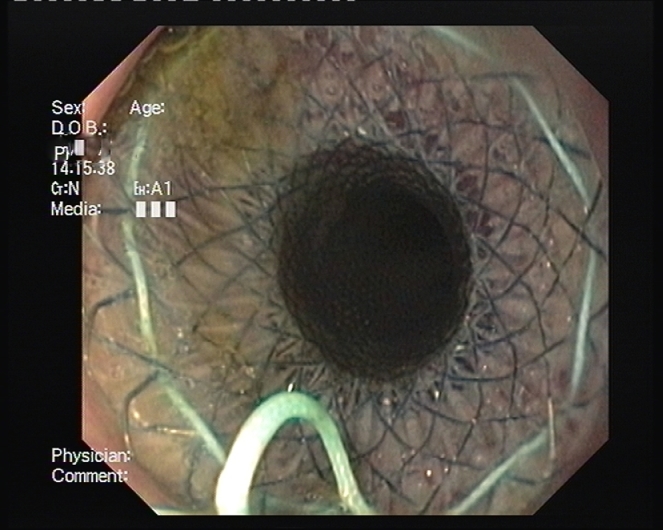
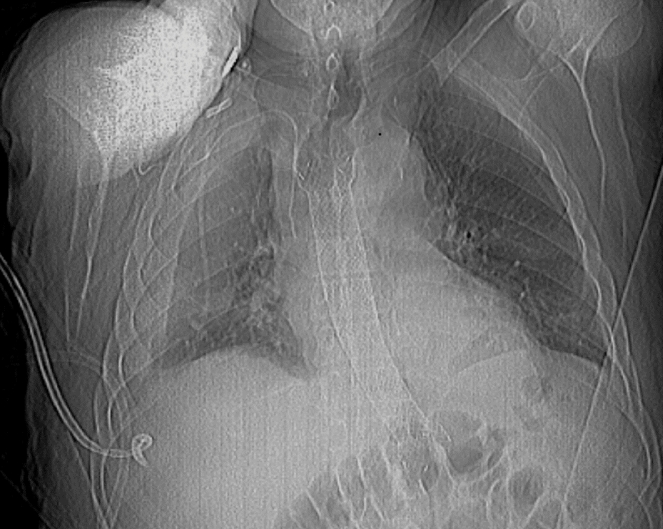
Boerhaave syndrome refers to a spontaneous perforation of the esophagus that results from severe straining or vomiting. This uncommon situation may lead to serious outcome with chemical mediastinitis, and is associated with high morbidity and mortality. Surgery, although associated with high morbidity and mortality remains the treatment of choice, whereas endoscopic management with stent placement is preserved to treat inoperable patients. Removal of the stent is generally recommended after 4-6 weeks. We report a case of an elderly patient who presented with a large complicated Boerhaave's mid-esophageal perforation, with a complete recovery after a 3-month treatment with a long esophageal stent.
Keywords: Boerhaave syndrome; Esophageal rupture; Esophageal stent.
Figures


References
-
- van Heel N.C., Haringsma J., Spaander M.C., Bruno M.J., Kuipers E.J. Short-term esophageal stenting in the management of benign perforations. Am J Gastroenterol. 2010;105(7):1515. - PubMed
-
- Freeman R.K., Ascioti A.J., Dake M., Mahidhara R.S. An assessment of the optimal time for removal of esophageal stents used in the treatment of an esophageal anastomotic leak or perforation. Ann Thorac Surg. 2015;100(2):422–428. - PubMed
-
- Schweigert M., Beattie R., Solymosi N., Booth K., Dubecz A., Muir A. Endoscopic stent insertion versus primary operative management for spontaneous rupture of the esophagus (Boerhaave syndrome): an international study comparing the outcome. Am Surg. 2013;79:634. - PubMed
-
- Dasari B.V., Neely D., Kennedy A., Spence G., Rice P., Mackle E. The role of esophageal stents in the management of esophageal anastomotic leaks and benign esophageal perforations. Ann Surg. 2014;259:852. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
