

High-resolution manometry is superior to endoscopy and radiology in assessing and grading sliding hiatal hernia: A comparison with surgical in vivo evaluation
- PMID: 30228885
- PMCID: PMC6137592
- DOI: 10.1177/2050640618769160
High-resolution manometry is superior to endoscopy and radiology in assessing and grading sliding hiatal hernia: A comparison with surgical in vivo evaluation
Abstract
Background: Hiatal hernia is diagnosed by barium-swallow esophagogram or esophagogastroduodenoscopy, with possible suboptimal results. High-resolution manometry clearly identifies crural diaphragm and lower esophageal sphincter.
Objectives: To assess the diagnostic accuracy of high-resolution manometry in detecting hiatal hernia compared to esophagogram and esophagogastroduodenoscopy, using as reference the surgical in vivo measurement.
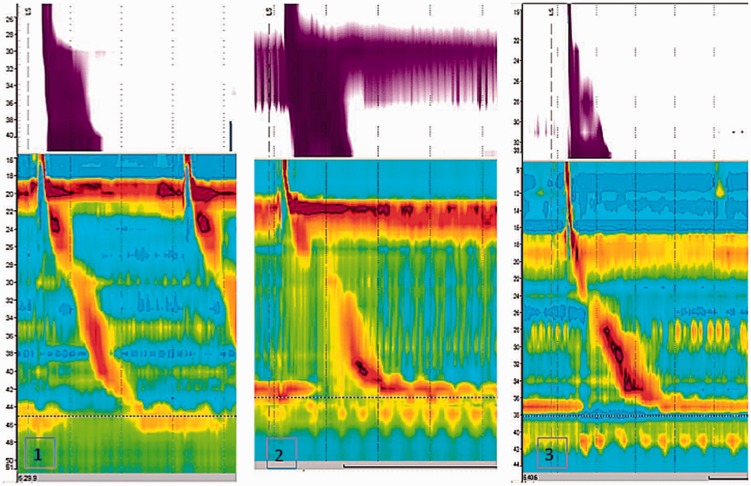
Methods: Patients were studied with esophagogram, esophagogastroduodenoscopy, high-resolution manometry and in vivo evaluation of the esophago-gastric junction. Esophago-gastric junction was classified as type I (no separation between crural diaphragm and lower esophageal sphincter); type II (≥1, ≤ 2 cm separation); type III (>2 cm). During in vivo measurement, distance between the esophago-gastric junction and crural diaphragm proximal border was recorded.
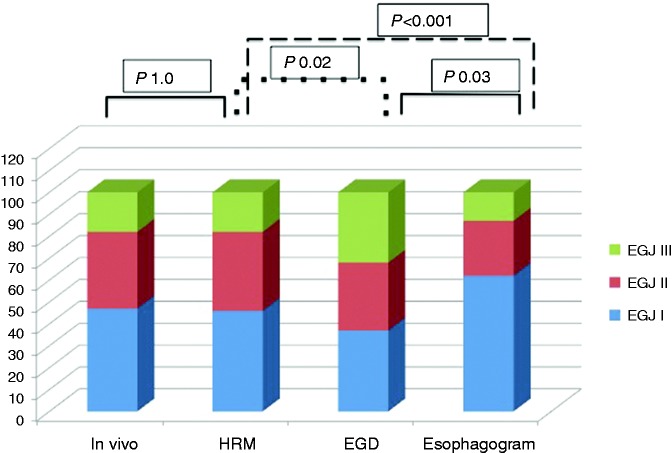
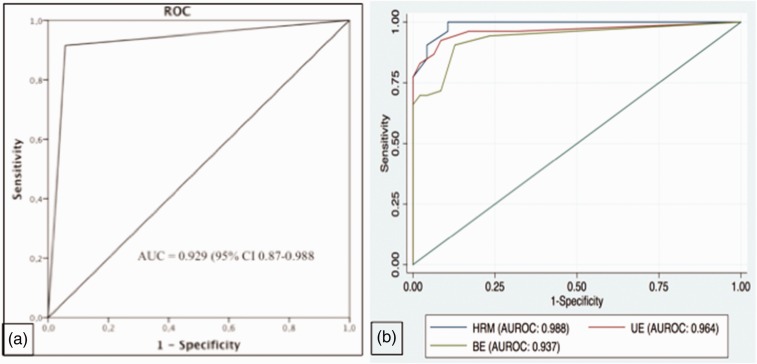
Results: Surgery identified 53 hiatal hernias in 100 patients. Forty-seven percent were classified as type I esophago-gastric junction, 35% type II and 18% type III. Referenced to in vivo evaluation, high-resolution manometry showed superior diagnostic sensitivity and specificity (94.3% and 91.5%, respectively) to esophagogram and esophagogastroduodenoscopy, with 92.6% predictive value of a positive test and 93.5% predictive value of a negative test. The kappa value for high-resolution manometry and in vivo evaluation was 0.85. High-resolution manometry showed optimal sensitivity and specificity in detecting types I, II and III esophago-gastric junction.
Conclusions: High-resolution manometry enables an accurate diagnosis of hiatal hernia and a better classification than endoscopy and radiology, reaching optimal agreement with in vivo assessment.
Keywords: Hiatal hernia; barium esophagogram; esophagogastric junction; high resolution manometry; upper endoscopy.
Figures

References
-
- Mittal RK, Balaban DH. The esophagogastric junction. N Engl J Med 1997; 336: 924–932. - PubMed
-
- Bredenoord AJ, Weusten BLAM, Timmer R, et al. Intermittent spatial separation of diaphragm and lower esophageal sphincter favors acidic and weakly acidic reflux. Gastroenterology 2006; 130: 334–340. - PubMed
-
- Savarino E, Zentilin P, Frazzoni M, et al. Characteristics of gastro-esophageal reflux episodes in Barrett's esophagus, erosive esophagitis and healthy volunteers. Neurogastroenterol Motil 2010; 22: 1061–e1280. - PubMed
-
- Savarino E, Gemignani L, Pohl D, et al. Oesophageal motility and bolus transit abnormalities increase in parallel with the severity of gastro-oesophageal reflux disease. Aliment Pharmacol Ther 2011; 34: 476–486. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
