

A Patient-Focused Technology-Enabled Program Improves Outcomes in Primary Total Hip and Knee Replacement Surgery
- PMID: 30229224
- PMCID: PMC6133096
- DOI: 10.2106/JBJS.OA.16.00023
A Patient-Focused Technology-Enabled Program Improves Outcomes in Primary Total Hip and Knee Replacement Surgery
Abstract
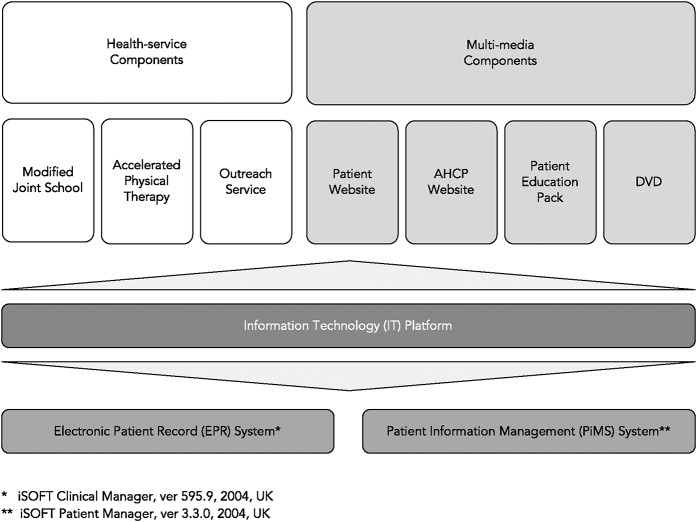
Background: A patient-engagement and pathway-management program for patients undergoing primary total hip and knee replacement was evaluated. Health-service and multimedia features supported by technology were integrated with existing enhanced recovery after surgery (ERAS) practices. The primary objective was to demonstrate the impact on length of stay. The secondary objective was to assess the impact on clinical, patient-focused, and financial outcomes.
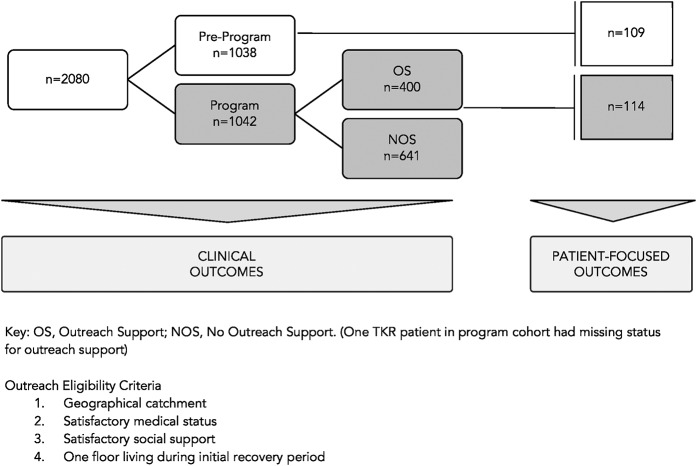
Methods: Two thousand and eighty consecutive patients undergoing primary total hip replacement (n = 1,034) and total knee replacement (n = 1,046) were classified into "pre-program" (retrospectively assessed [n = 1,038]) and "program" (prospectively assessed [n = 1,042]) cohorts. Patients in the program cohort were subdivided according to those who were eligible for criteria-based outreach support (OS) (n = 401) and those who were ineligible for this service (NOS) (n = 641). Clinical outcomes were assessed for all patients, and patient-focused outcomes were assessed for a subset (n = 223).
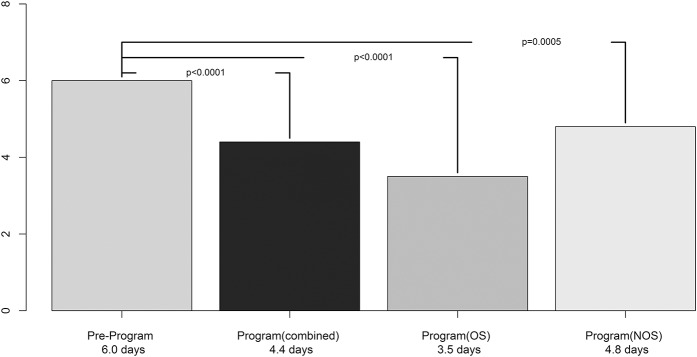
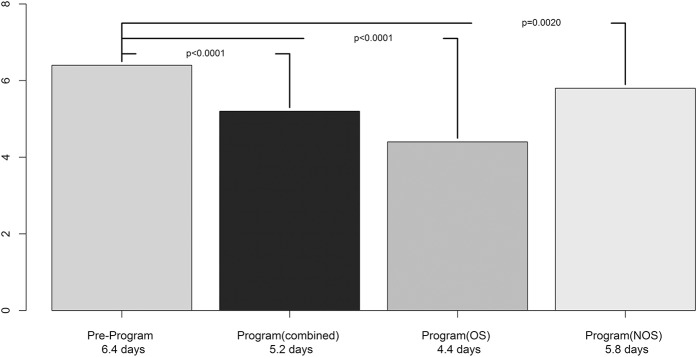
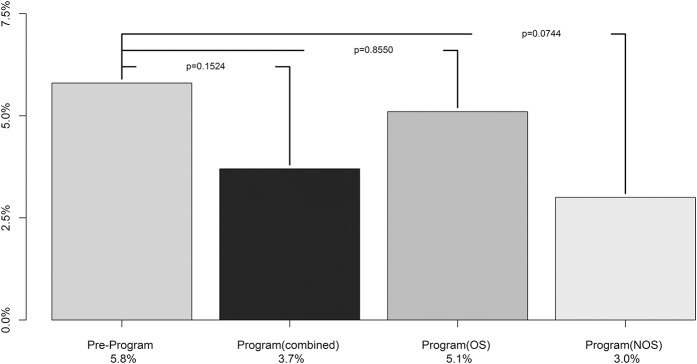
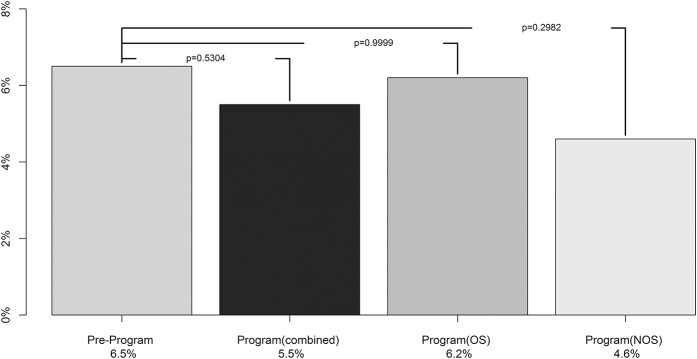
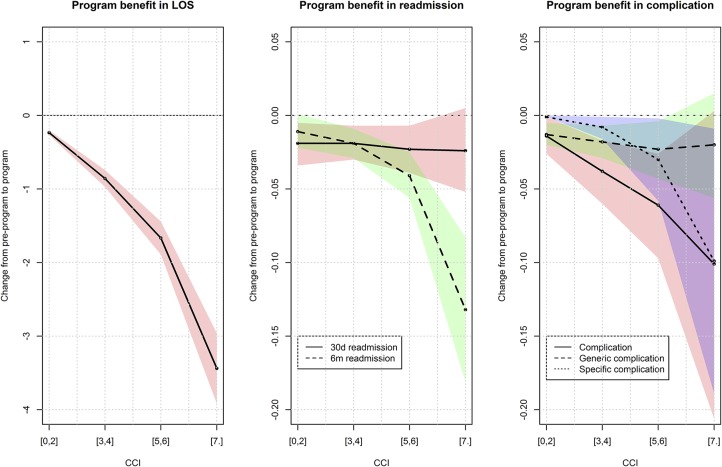
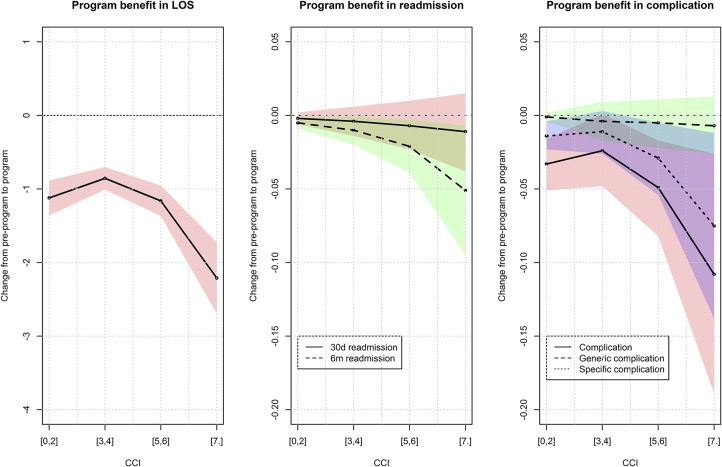
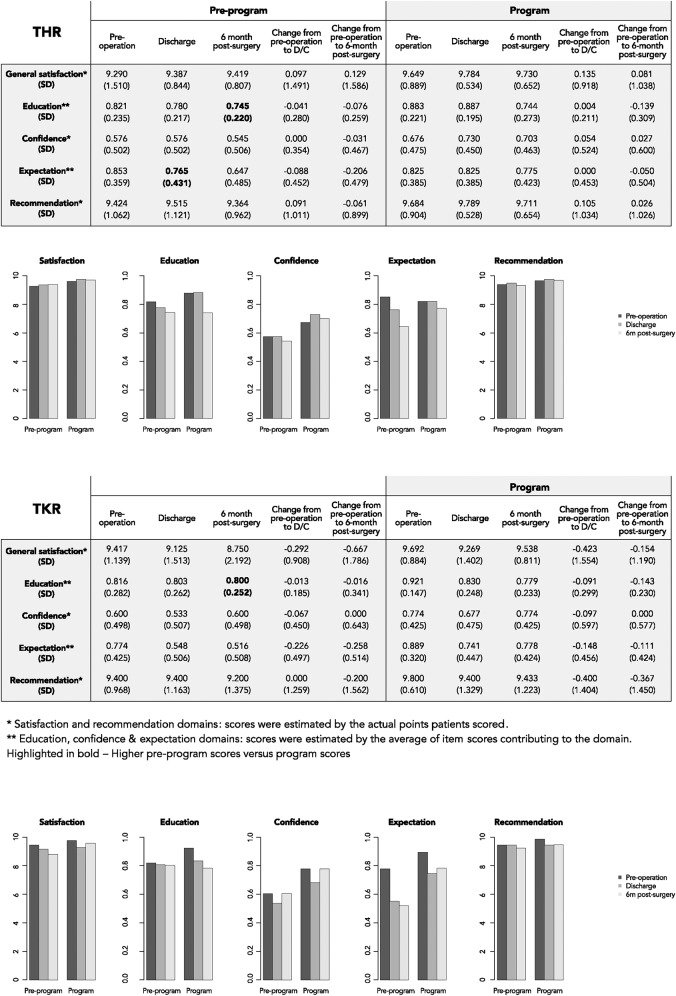
Results: The mean reduction in length of stay ranged from 20% (1.2 days) to 42% (2.5 days) following total hip replacement and from 9% (0.6 day) to 31% (2 days) following total knee replacement (p < 0.001). Clinical outcomes (readmissions, complications, emergency department re-attendance rates) were not significantly negatively impacted. The Oxford Hip Score had numerically larger improvement after total hip replacement in the OS group than in the pre-program group (4.1-point increase), and the Oxford Knee Score had numerically larger improvement after total knee replacement in the NOS group than in the pre-program group (0.8-point increase). The patients in the program cohort (either OS or NOS) rated overall health gain as higher than those in the pre-program cohort (gain in numerical rating scale, 1.4 points for patients managed with total hip replacement, 0.6 points for patients managed with total knee replacement). Older patients and those with higher comorbidity indices benefited most with respect to length of stay and multiple clinical outcomes. Patient experience was significantly improved across domains (p < 0.001 to p = 0.003). Potential savings for patients managed with total hip replacement (£401.64 [$267.76] per patient) exceeded estimated program charges of £50 [$33.33] to £60 [$40] per patient, whereas the potential savings for patients managed with total knee replacement (£76.67 [$51.11] per patient) were sufficient to achieve a reduction of total system costs.
Conclusions: Technology-enabled programs may deliver enhanced care at lower costs for patients undergoing lower-limb arthroplasty. Shorter durations of inpatient stay without a negative impact on clinical outcomes and improved patient-focused outcomes and experience can deliver substantial value that can be especially beneficial for older patients and those with greater medical complexity.
Level of evidence: Therapeutic Level III. See Instructions for Authors for a complete description of levels of evidence.
Figures
Similar articles
-
Enhanced recovery after surgery (ERAS) in hip and knee replacement surgery: description of a multidisciplinary program to improve management of the patients undergoing major orthopedic surgery.Musculoskelet Surg. 2020 Apr;104(1):87-92. doi: 10.1007/s12306-019-00603-4. Epub 2019 May 3. Musculoskelet Surg. 2020. PMID: 31054080
-
Enhanced recovery short-stay hip and knee joint replacement program improves patients outcomes while reducing hospital costs.Orthop Traumatol Surg Res. 2019 Nov;105(7):1237-1243. doi: 10.1016/j.otsr.2019.08.013. Epub 2019 Oct 3. Orthop Traumatol Surg Res. 2019. PMID: 31588036
-
Enhanced Recovery After Surgery for Hip and Knee Replacements.Orthop Nurs. 2017 May/Jun;36(3):203-210. doi: 10.1097/NOR.0000000000000351. Orthop Nurs. 2017. PMID: 28538534
-
Fast-track hip and knee arthroplasty: clinical and organizational aspects.Acta Orthop Suppl. 2012 Oct;83(346):1-39. doi: 10.3109/17453674.2012.700593. Acta Orthop Suppl. 2012. PMID: 23205862 Review.
-
Developing an enhanced recovery after surgery program for oncology patients who undergo hip or knee reconstruction surgery.World J Orthop. 2021 Jun 18;12(6):346-359. doi: 10.5312/wjo.v12.i6.346. eCollection 2021 Jun 18. World J Orthop. 2021. PMID: 34189073 Free PMC article. Review.
Cited by
-
Comparison of a Smartphone App to Manual Knee Range of Motion Measurements.Arthroplast Today. 2022 Apr 4;15:43-46. doi: 10.1016/j.artd.2021.09.005. eCollection 2022 Jun. Arthroplast Today. 2022. PMID: 35399987 Free PMC article.
-
The factors determining early mobilization in elderly patients undergoing total knee replacement.BMC Geriatr. 2025 Feb 20;25(1):118. doi: 10.1186/s12877-025-05772-5. BMC Geriatr. 2025. PMID: 39979824 Free PMC article.
-
Patient Engagement Approaches in Total Joint Arthroplasty: A Review of Two Decades.J Patient Exp. 2021 Aug 19;8:23743735211036525. doi: 10.1177/23743735211036525. eCollection 2021. J Patient Exp. 2021. PMID: 34435090 Free PMC article.
-
Enhanced recovery after surgery (ERAS) in sacral tumour surgery and comprehensive description of a multidisciplinary program: a prospective study in a specialized hospital in China.Int Orthop. 2024 Feb;48(2):581-601. doi: 10.1007/s00264-023-06016-0. Epub 2023 Nov 15. Int Orthop. 2024. PMID: 37966532
-
Using Patient Engagement Platforms in the Postoperative Management of Patients.Curr Rev Musculoskelet Med. 2020 Aug;13(4):479-484. doi: 10.1007/s12178-020-09638-8. Curr Rev Musculoskelet Med. 2020. PMID: 32388724 Free PMC article. Review.
References
-
- Hansson T, Hansson E, Malchau H. Utility of spine surgery: a comparison of common elective orthopaedic surgical procedures. Spine. 2008. December 01;33(25):2819-30. - PubMed
-
- Jenkins PJ, Clement ND, Hamilton DF, Gaston P, Patton JT, Howie CR. Predicting the cost-effectiveness of total hip and knee replacement: a health economic analysis. Bone Joint J. 2013. January;95-B(1):115-21. - PubMed
-
- National Joint Registry for England. Wales, Northern Ireland, and the Isle of Man. 11th annual report of the National Joint Registry. http://www.njrcentre.org.uk/njrcentre/Portals/0/Documents/England/Report...
-
- Norman-Taylor FH, Palmer CR, Villar RN. Quality-of-life improvement compared after hip and knee replacement. J Bone Joint Surg Br. 1996. January;78(1):74-7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials