

Burden, Prevalence, and Treatment of Uterine Fibroids: A Survey of U.S. Women
- PMID: 30230950
- PMCID: PMC6247381
- DOI: 10.1089/jwh.2018.7076
Burden, Prevalence, and Treatment of Uterine Fibroids: A Survey of U.S. Women
Abstract
Background: Most women will experience uterine fibroids by the age of 50, yet few data exist describing the overall patient experience with fibroids. The objective of this population-based survey was to characterize symptom burden, patient awareness, and treatment decision-making for fibroids, including a comparison among women of varying backgrounds.
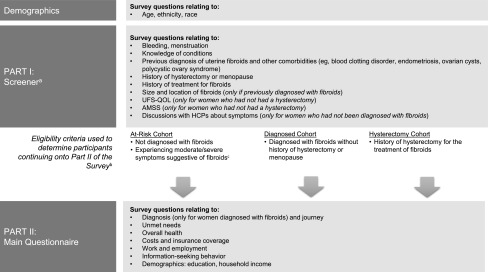
Materials and methods: Women (≥18 years) were recruited via email from GfK KnowledgePanel®, a representative panel of US households, or identified with opt-in consumer panels. The Uterine Fibroid Symptom and Health-Related Quality of Life (UFS-QOL) questionnaire and Aberdeen Menorrhagia Severity Scale (AMSS) were included.
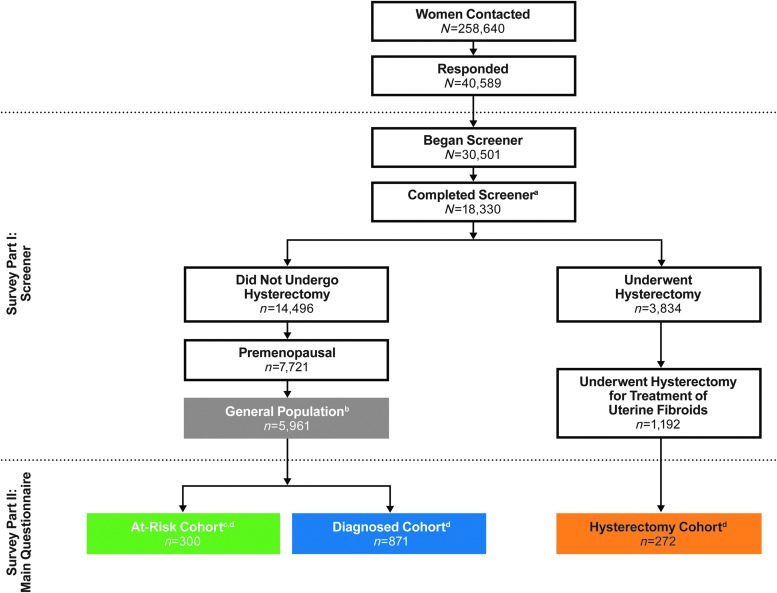
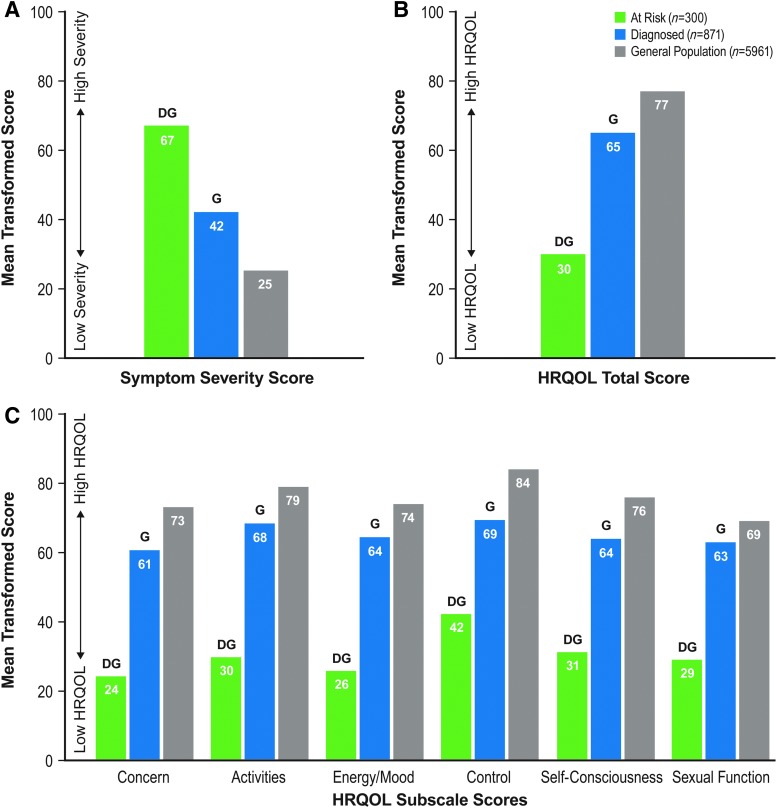
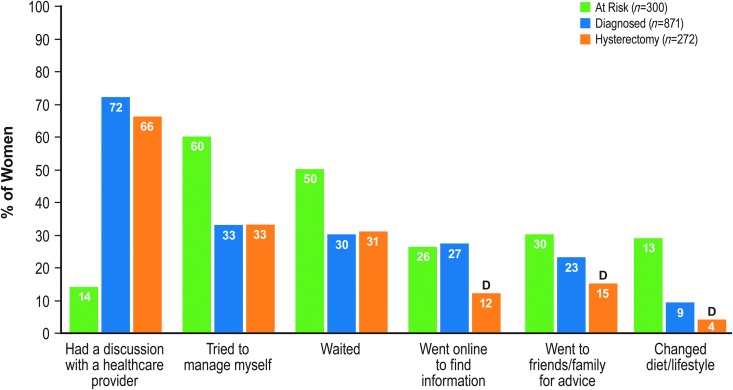
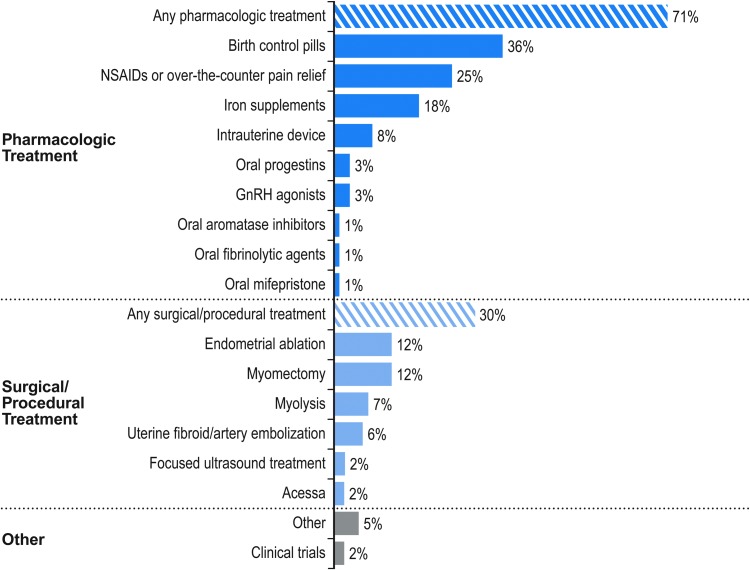
Results: Eligible women were grouped into three cohorts: "at-risk" (symptoms suggestive of fibroids without clinical diagnosis, n = 300), "diagnosed" (n = 871), and fibroid-related "hysterectomy" (n = 272). Cohort and intracohort race/ethnicity and income analyses revealed differences in symptom burden, awareness/perception, and treatment history. Based on UFS-QOL scores, at-risk women reported significantly greater symptom severity and decreased health-related QOL versus diagnosed women; Hispanic women reported greater symptom severity versus white and black women. At-risk women also reported heavy menstrual bleeding and significant impact on work productivity. Among diagnosed women, 71% used pharmacologic therapy for symptom relief, and 30% underwent surgical or procedural treatment. Initial discussions with healthcare providers significantly impacted treatment outcomes; the hysterectomy cohort was most likely to first discuss hysterectomy.
Conclusions: Women with fibroids or symptoms suggestive of fibroids experience significant distress that reduces QOL, particularly racial minorities and women in lower income brackets. Survey results suggest that many women are likely undiagnosed, underscoring the need for improved awareness and education.
Keywords: burden; health disparities; quality of life; race/ethnicity; uterine fibroids; work.
Conflict of interest statement
Erica Marsh is a consultant for Allergan plc and AbbVie. Ayman Al-Hendy is a consultant for Allergan plc, Bayer, Repros, and AbbVie. Dale Kappus was an employee of GfK at time of study. Dale Kappus is currently employed by Time Inc. in a noneditorial capacity—she coauthored the article in a personal capacity, any opinions are her own, and Time Inc. is not in any way affiliated. Alex Galitsky is an employee of GfK. Elizabeth A. Stewart received grant funding from the National Institutes of Health. Dr. Stewart has also served as a consultant/on advisory boards for AbbVie, Allergan, Astellas Pharma, Bayer Healthcare, Glaxo Smith Kline, Gynesonics, Myovant, and Welltwigs. Majid Kerolous is an employee of Allergan plc.
Figures
References
-
- Drayer SM, Catherino WH. Prevalence, morbidity, and current medical management of uterine leiomyomas. Int J Gynaecol Obstet 2015;131:117–122 - PubMed
-
- Stewart EA, Cookson C, Gandolfo RA, Schulze-Rath R. Epidemiology of uterine fibroids: A systematic review. BJOG 2017;124:1501–1512 - PubMed
-
- Stewart EA, Laughlin-Tommaso SK, Catherino WH, Lalitkumar S, Gupta D, Vollenhoven B. Uterine fibroids. Nat Rev Dis Primers 2016;2:16043. - PubMed
-
- Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: Ultrasound evidence. Am J Obstet Gynecol 2003;188:100–107 - PubMed
-
- Bartels CB, Cayton KC, Chuong FS, et al. An evidence-based approach to the medical management of fibroids: A systematic review. Clin Obstet Gynecol 2016;59:30–52 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
