

Body Temperature, Heart Rate, and Short-Term Outcome of Cooled Infants
- PMID: 30230963
- PMCID: PMC6434598
- DOI: 10.1089/ther.2018.0019
Body Temperature, Heart Rate, and Short-Term Outcome of Cooled Infants
Abstract
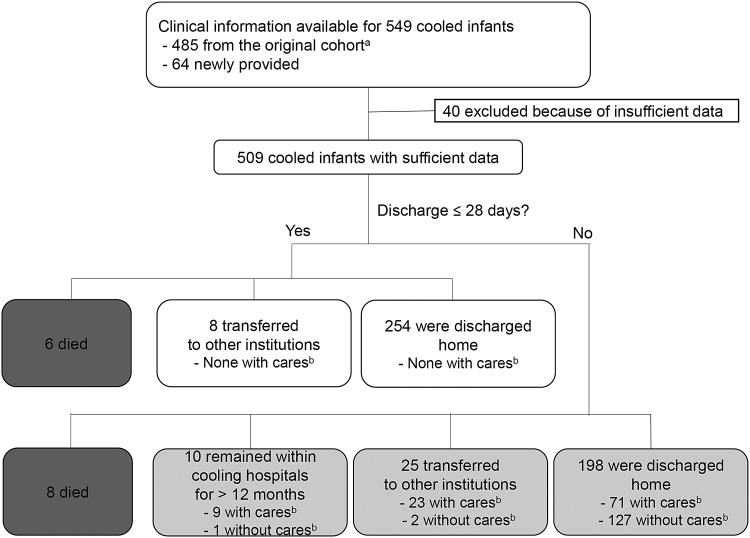
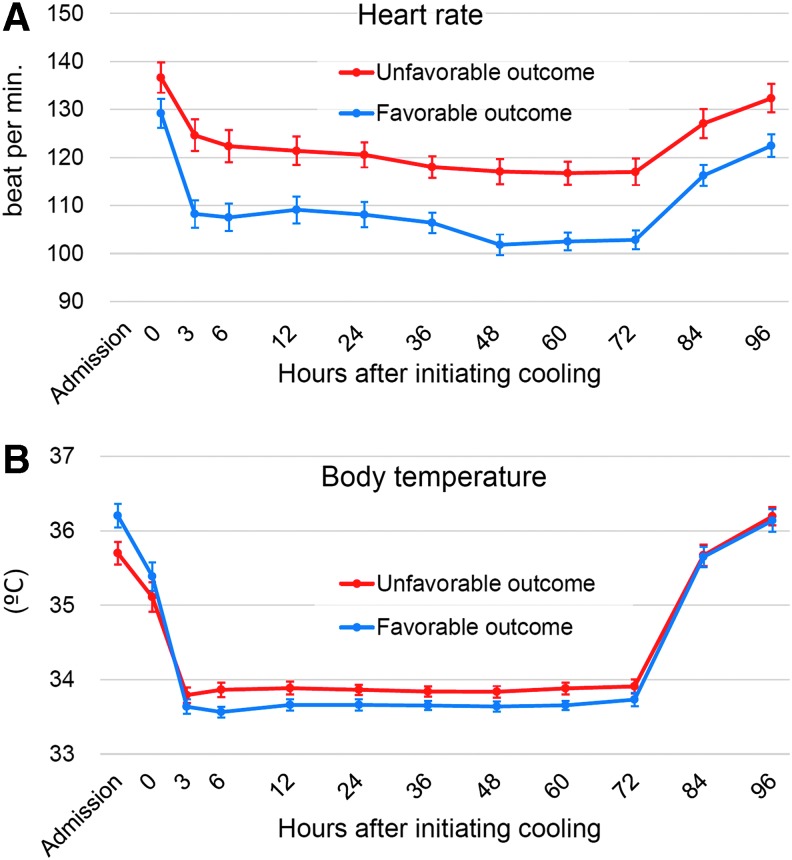
Therapeutic hypothermia following neonatal encephalopathy is neuroprotective. However, approximately one in two cooled infants still die or develop permanent neurological impairments. Further understanding of variables associated with the effectiveness of cooling is important to improve the therapeutic regimen. To identify clinical factors associated with short-term outcomes of cooled infants, clinical data of 509 cooled infants registered to the Baby Cooling Registry of Japan between 2012 and 2014 were evaluated. Independent variables of death during the initial hospitalization and survival discharge from the cooling hospital at ≤28 days of life were assessed. Death was associated with higher Thompson scores at admission (p < 0.001); higher heart rates after 3-72 hours of cooling (p < 0.001); and higher body temperature after 24 hours of cooling (p = 0.002). Survival discharge was associated with higher 10 minutes Apgar scores (p < 0.001); higher blood pH and base excess (both p < 0.001); lower Thompson scores (at admission and after 24 hours of cooling; both p < 0.001); lower heart rates at initiating cooling (p = 0.003) and after 24 hours of cooling (p < 0.001) and lower average values after 3-72 hours of cooling (p < 0.001); higher body temperature at admission (p < 0.001); and lower body temperature after 24 hours and lower mean values after 3-72 hours of cooling (both p < 0.001). Survival discharge was best explained by higher blood pH (p < 0.05), higher body temperature at admission (p < 0.01), and lower body temperature and heart rate after 24 hours of cooling (p < 0.01 and <0.001, respectively). Lower heart rate, higher body temperature at admission, and lower body temperature during cooling were associated with favorable short-term outcomes.
Keywords: body temperature; heart rate; selective-head cooling; therapeutic hypothermia; whole-body cooling.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Azzopardi D, Strohm B, Marlow N, Brocklehurst P, Deierl A, Eddama O, Goodwin J, Halliday HL, Juszczak E, Kapellou O, Levene M, Linsell L, Omar O, Thoresen M, Tusor N, Whitelaw A, Edwards AD. Effects of hypothermia for perinatal asphyxia on childhood outcomes. N Engl J Med 2014;371:140–149 - PubMed
-
- Basu SK, Salemi JL, Gunn AJ, Kaiser JR. Hyperglycaemia in infants with hypoxic-ischaemic encephalopathy is associated with improved outcomes after therapeutic hypothermia: a post hoc analysis of the CoolCap Study. Arch Dis Child Fetal Neonatal Ed 2017;102:F299–F306 - PubMed
-
- Chandrasekaran M, Chaban B, Montaldo P, Thayyil S. Predictive value of amplitude-integrated EEG (aEEG) after rescue hypothermic neuroprotection for hypoxic ischemic encephalopathy: a meta-analysis. J Perinatol 2017;37:684–689 - PubMed
-
- Chouthai NS, Sobczak H, Khan R, Subramanian D, Raman S, Rao R. Hyperglycemia is associated with poor outcome in newborn infants undergoing therapeutic hypothermia for hypoxic ischemic encephalopathy. J Neonatal Perinatal Med 2015;8:125–131 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical