

Predicting treatment Response based on Dual assessment of magnetic resonance Imaging kinetics and Circulating Tumor cells in patients with Head and Neck cancer (PREDICT-HN): matching 'liquid biopsy' and quantitative tumor modeling
- PMID: 30231854
- PMCID: PMC6148797
- DOI: 10.1186/s12885-018-4808-5
Predicting treatment Response based on Dual assessment of magnetic resonance Imaging kinetics and Circulating Tumor cells in patients with Head and Neck cancer (PREDICT-HN): matching 'liquid biopsy' and quantitative tumor modeling
Abstract
Background: Magnetic resonance imaging (MRI) has improved capacity to visualize tumor and soft tissue involvement in head and neck cancers. Using advanced MRI, we can interrogate cell density using diffusion weighted imaging, a quantitative imaging that can be used during radiotherapy, when diffuse inflammatory reaction precludes PET imaging, and can assist with target delineation as well. Correlation of circulating tumor cells (CTCs) measurements with 3D quantitative tumor characterization could potentially allow selective, patient-specific response-adapted escalation or de-escalation of local therapy, and improve the therapeutic ratio, curing the greatest number of patients with the least toxicity.
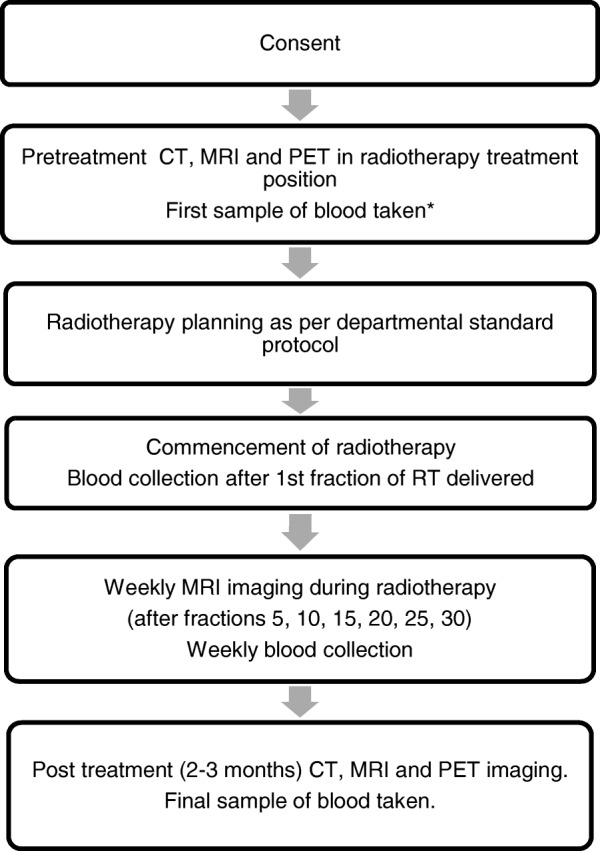
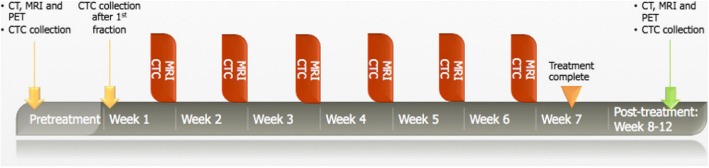
Methods: The proposed study is designed as a prospective observational study and will collect pretreatment CT, MRI and PET/CT images, weekly serial MR imaging during RT and post treatment CT, MRI and PET/CT images. In addition, blood sample will be collected for biomarker analysis at those time intervals. CTC assessments will be performed on the CellSave tube using the FDA-approved CellSearch® Circulating Tumor Cell Kit (Janssen Diagnostics), and plasma from the EDTA blood samples will be collected, labeled with a de-identifying number, and stored at - 80 °C for future analyses.
Discussion: The primary objective of the study is to evaluate the prognostic value and correlation of weekly tumor response kinetics (gross tumor volume and MR signal changes) and circulating tumor cells of mucosal head and neck cancers during radiation therapy using MRI in predicting treatment response and clinical outcomes. This study will provide landmark information as to the utility of CTCs ('liquid biopsy) and tumor-specific functional quantitative imaging changes during treatment to guide personalization of treatment for future patients. Combining the biological information from CTCs and the structural information from MRI may provide more information than either modality alone. In addition, this study could potentially allow us to determine the optimal time to obtain MR imaging and/ or CTCs during radiotherapy to assess tumor response and provide guidance for patient selection and stratification for future dose escalation or de-escalation strategies.
Trial registration: Clinicaltrials.gov ( NCT03491176 ). Date of registration: 9th April 2018. (retrospectively registered). Date of enrolment of the first participant: 30th May 2017.
Keywords: Biomarker; Circulating tumor cells; Head and neck cancer; Magnetic resonance imaging.
Conflict of interest statement
Ethics approval and consent to participate
This study is in accordance with the Declaration of Helsinki and has been approved by the Institutional Review Board at the University of Texas MD Anderson Cancer Center. The study is registered on
Patients within the institution, who are scheduled for definitive radiotherapy, will be identified by either an attending physician or research fellow in the Department of Radiation Oncology. During clinic appointments, potential subjects will be informed of their eligibility and asked if they would be interested in research participation. In the privacy of the exam room, the treating physician or research fellow will discuss all aspects of the study with potential subjects and answer any questions. Interested subjects then have a consent interview with the research nurse or research data coordinator in the exam room or other private area (i.e. patient education/consultation room). Subjects will be given a copy of the Informed Consent and will be further instructed about the study and the elements of the consent document. The subject will be given as much time as needed to review and discuss the study and consent and the research nurse or research data coordinator will answer any remaining questions. The treating physician is also available to address any questions or concerns the subject may have. Subjects who agree to participate will sign the protocol-specific informed consent. Non-English speaking patients will be consented using an MD Anderson Translator and a verbal translation preparative sheet using MD Anderson policies for Informed Consent translation in that patient’s primary language. Once two patients have been consented in a given language, the research nurse or research data coordinator will request institutional translation of the entire consent into that language. Patients may withdraw from the study at any time without any penalty. If a patient withdraws, any blood or tissue not already used will not be used for further studies.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Multiparametric magnetic resonance imaging in mucosal primary head and neck cancer: a prospective imaging biomarker study.BMC Cancer. 2017 Jul 10;17(1):475. doi: 10.1186/s12885-017-3448-5. BMC Cancer. 2017. PMID: 28693449 Free PMC article.
-
Correlation of Circulating Tumor Cell Measurements with 3D Quantitative Tumor Characterization to Predict Clinical Outcomes in Cancer.Methods Mol Biol. 2021;2174:135-141. doi: 10.1007/978-1-0716-0759-6_9. Methods Mol Biol. 2021. PMID: 32813248
-
Application of circulating tumour cells to predict response to treatment in head and neck cancer.Cell Oncol (Dordr). 2022 Aug;45(4):543-555. doi: 10.1007/s13402-022-00681-w. Epub 2022 Jun 23. Cell Oncol (Dordr). 2022. PMID: 35737211 Free PMC article.
-
Circulating tumor cells as biomarkers in head and neck cancer: recent advances and future outlook.Expert Rev Mol Diagn. 2018 Oct;18(10):897-906. doi: 10.1080/14737159.2018.1522251. Epub 2018 Sep 21. Expert Rev Mol Diagn. 2018. PMID: 30199647 Review.
-
[Role and responsibility of multimodal imaging in head and neck cancer].Magy Onkol. 2013 Sep;57(3):182-202. Epub 2013 Sep 20. Magy Onkol. 2013. PMID: 24107825 Review. Hungarian.
Cited by
-
Detection of circulating tumor cells in patients with laryngeal cancer using ScreenCell: Comparative pre- and post-operative analysis and association with prognosis.Oncol Lett. 2020 Jun;19(6):4183-4188. doi: 10.3892/ol.2020.11528. Epub 2020 Apr 10. Oncol Lett. 2020. PMID: 32391112 Free PMC article.
-
Immunobiology of cancer stem cells and their immunoevasion mechanisms.Mol Biol Rep. 2023 Nov;50(11):9559-9573. doi: 10.1007/s11033-023-08768-9. Epub 2023 Sep 30. Mol Biol Rep. 2023. PMID: 37776412 Review.
-
Changes in Apparent Diffusion Coefficient (ADC) in Serial Weekly MRI during Radiotherapy in Patients with Head and Neck Cancer: Results from the PREDICT-HN Study.Curr Oncol. 2022 Aug 31;29(9):6303-6313. doi: 10.3390/curroncol29090495. Curr Oncol. 2022. PMID: 36135064 Free PMC article.
-
Circulating Tumour Cell Biomarkers in Head and Neck Cancer: Current Progress and Future Prospects.Cancers (Basel). 2019 Aug 5;11(8):1115. doi: 10.3390/cancers11081115. Cancers (Basel). 2019. PMID: 31387228 Free PMC article. Review.
-
Circulating p16-Positive and p16-Negative Tumor Cells Serve as Independent Prognostic Indicators of Survival in Patients with Head and Neck Squamous Cell Carcinomas.J Pers Med. 2021 Nov 7;11(11):1156. doi: 10.3390/jpm11111156. J Pers Med. 2021. PMID: 34834510 Free PMC article.
References
-
- Chaturvedi A, Engels E, Pfeiffer R, Hernandez BY, Xiao W, Kim E, Jiang B, Goodman M, Sibug-Saber M, Cozen W, Liu L, Lynch C, Wentzensen N, Jordan R, Altekruse S, Anderson WF, Rosenberg P, Gillison ML. Human papillomavirus (hpv) and rising oropharyngeal cancer incidence and survival in the United States. J Clin Oncol. 2011;29:5529. doi: 10.1200/jco.2011.29.15_suppl.5529. - DOI - PMC - PubMed
-
- Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tan PF, Westra WH, Chung CH, Jordan RC, Lu C, Kim H, Axelrod R, Silverman CC, Redmond KP, Gillison ML. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010;363:24–35. doi: 10.1056/NEJMoa0912217. - DOI - PMC - PubMed
-
- Campbell SR, Mohamed AS, Heukelom J, Awan MJ, Garden AS, Gunn GB, Rosenthal DI, Fuller CD. Primary tumor regression index: the prognostic value of volumetric image guided radiation therapy for head and neck cancer. Int J Radiat Oncol Biol Phys. 2016;96:E363–E364. doi: 10.1016/j.ijrobp.2016.06.1544. - DOI
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
