

Cost-effectiveness of pre-operative Staphylococcus aureus screening and decolonization
- PMID: 30231943
- PMCID: PMC8559732
- DOI: 10.1017/ice.2018.228
Cost-effectiveness of pre-operative Staphylococcus aureus screening and decolonization
Abstract
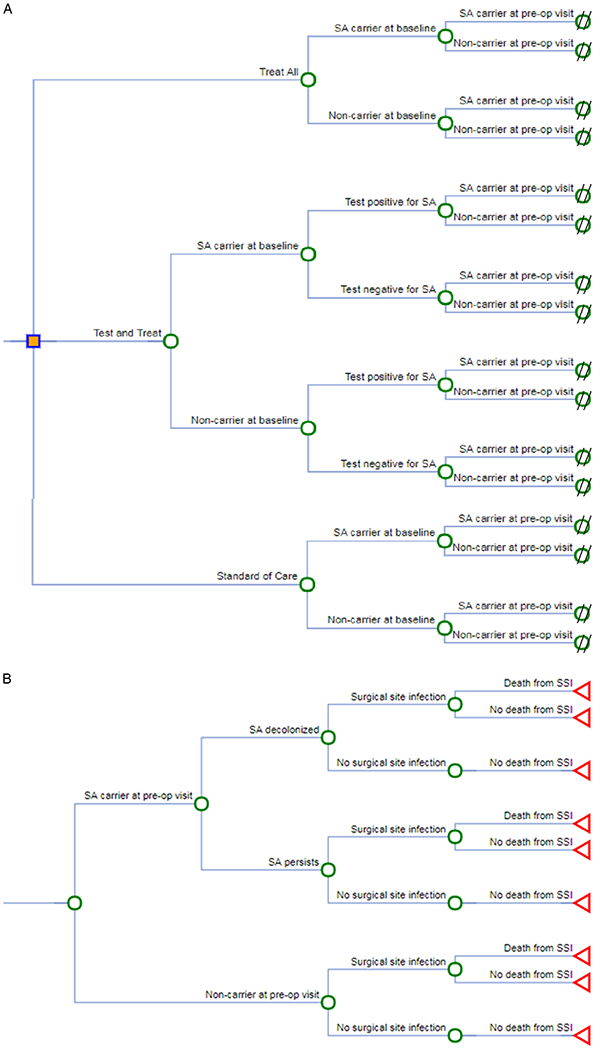
Objective: We developed a decision analytic model to evaluate the impact of a preoperative Staphylococcus aureus decolonization bundle on surgical site infections (SSIs), health-care-associated costs (HCACs), and deaths due to SSI.
Methods: Our model population comprised US adults undergoing elective surgery. We evaluated 3 self-administered preoperative strategies: (1) the standard of care (SOC) consisting of 2 disinfectant soap showers; (2) the "test-and-treat" strategy consisting of the decolonization bundle including chlorhexidine gluconate (CHG) soap, CHG mouth rinse, and mupirocin nasal ointment for 5 days) if S. aureus was found at any of 4 screened sites (nasal, throat, axillary, perianal area), otherwise the SOC; and (3) the "treat-all" strategy consisting of the decolonization bundle for all patients, without S. aureus screening. Model parameters were derived primarily from a randomized controlled trial that measured the efficacy of the decolonization bundle for eradicating S. aureus.
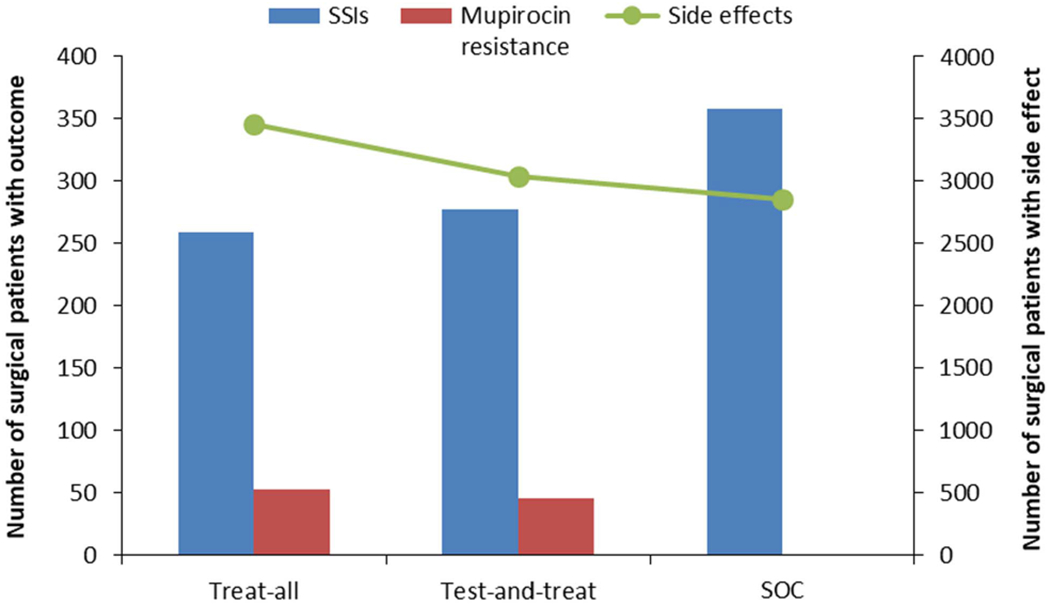
Results: Under base-case assumptions, the treat-all strategy yielded the fewest SSIs and the lowest HCACs, followed by the test-and-treat strategy. In contrast, the SOC yielded the most SSIs and the highest HCACs. Consequently, relative to the SOC, the average savings per operation was $217 for the treat-all strategy and $123 for the test-and-treat strategy, and the average savings per per SSI prevented was $21,929 for the treat-all strategy and $15,166 for the test-and-treat strategy. All strategies were sensitive to the probability of acquiring an SSI and the increased risk if SSI if the patient was colonized with SA.
Conclusion: We predict that the treat-all strategy would be the most effective and cost-saving strategy for preventing SSIs. However, because this strategy might select more extensively for mupirocin-resistant S. aureus and cause more medication adverse effects than the test-and-treat approach or the SOC, additional studies are needed to define its comparative benefits and harms.
Conflict of interest statement
Figures
References
-
- Hidron A, Edwards J, Patel J, et al. NHSN annual update: antimicrobial-resistant pathogens associated with healthcare-associated infections: annual summary of data reported to the National Healthcare Safety Network at the Centers for Disease Control and Prevention, 2006–2007. Infect Control Hosp Epidemiol 2008;29:996–1011. - PubMed
-
- Perl TM, Golub JE. New approaches to reduce Staphylococcus aureus nosocomial infection rates: treating S. aureus nasal carriage. Ann Pharmacother 1998;32:S7–S16. - PubMed
-
- Wenzel RP, Perl TM. The significance of nasal carriage of Staphylococcus aureus and the incidence of postoperative wound infections. J Hosp Infect 1995;31:13–24. - PubMed
-
- Ban KA, Minei JP, Laronga C, et al. American college of surgeons and surgical infection society: surgical site infection guidelines, 2016 update. Am Coll Surg 2017;224:59–74. - PubMed
-
- Global guidelines for the prevention of surgical site infection. World Health Organization; website. http://www.who.int/gpsc/ssi-guidelines/en/. Published 2016. Accessed July 21, 2017. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
