

IL-33 modulates inflammatory brain injury but exacerbates systemic immunosuppression following ischemic stroke
- PMID: 30232272
- PMCID: PMC6237219
- DOI: 10.1172/jci.insight.121560
IL-33 modulates inflammatory brain injury but exacerbates systemic immunosuppression following ischemic stroke
Abstract
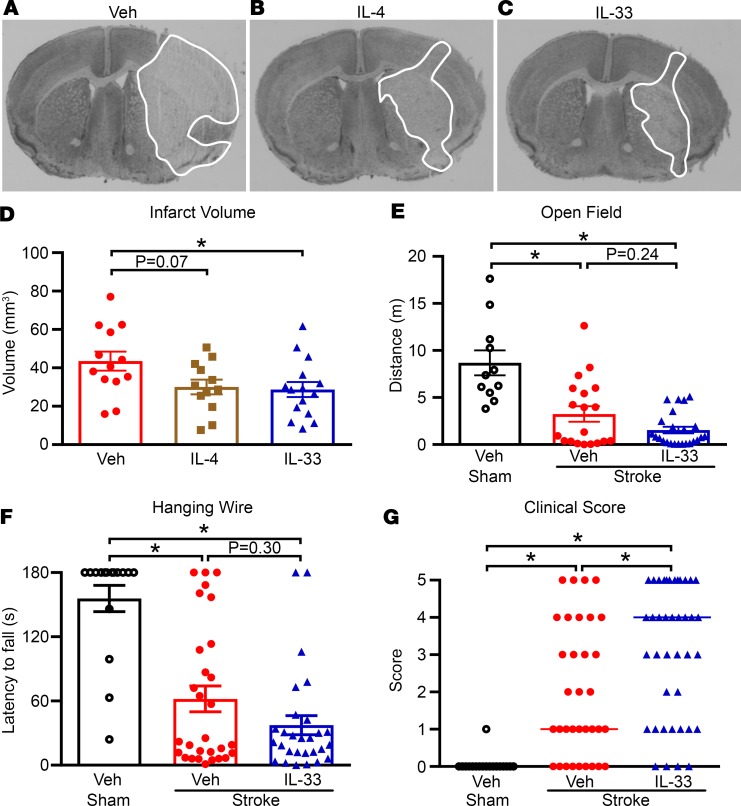
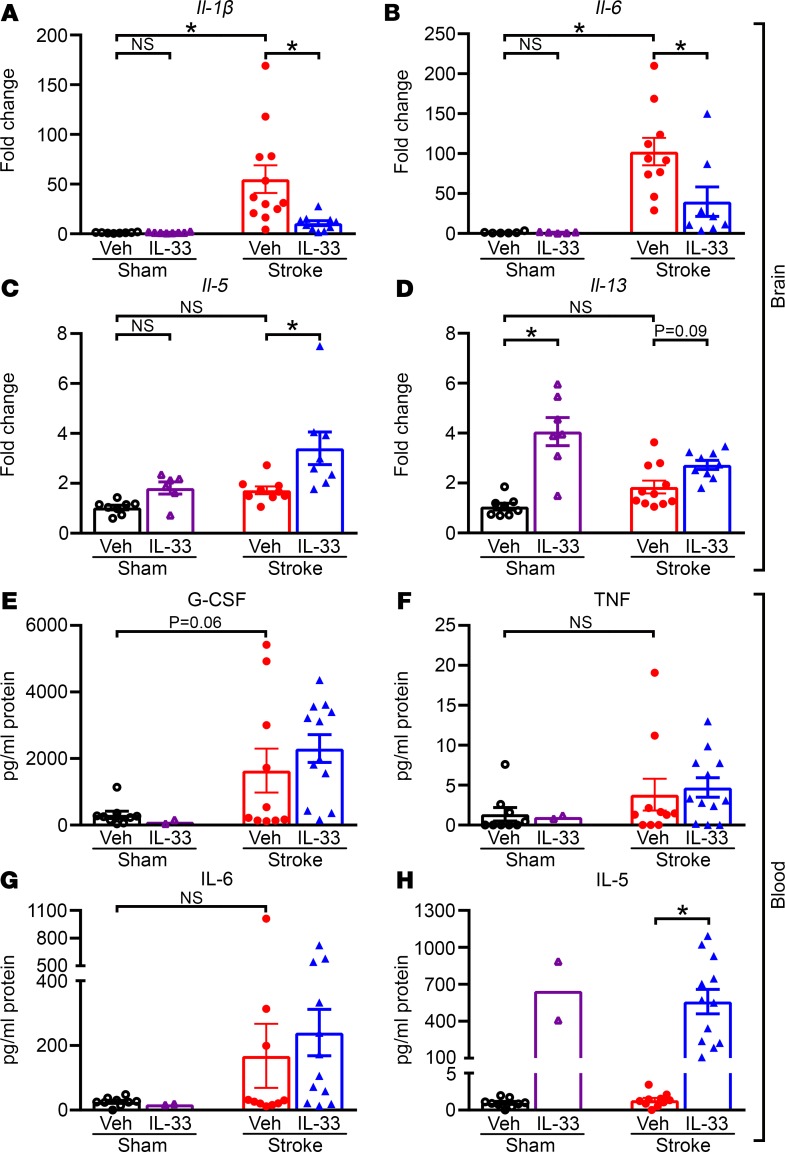
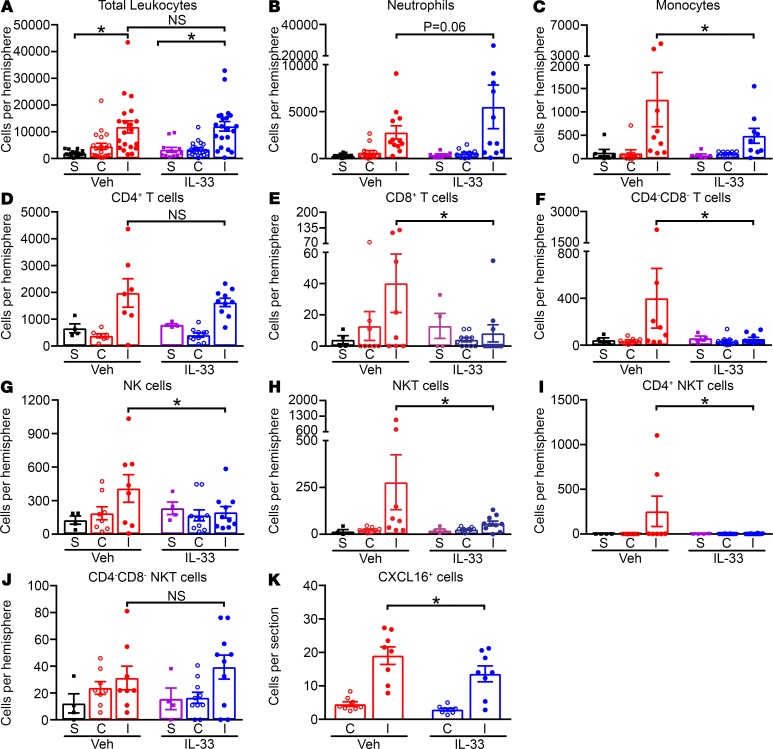
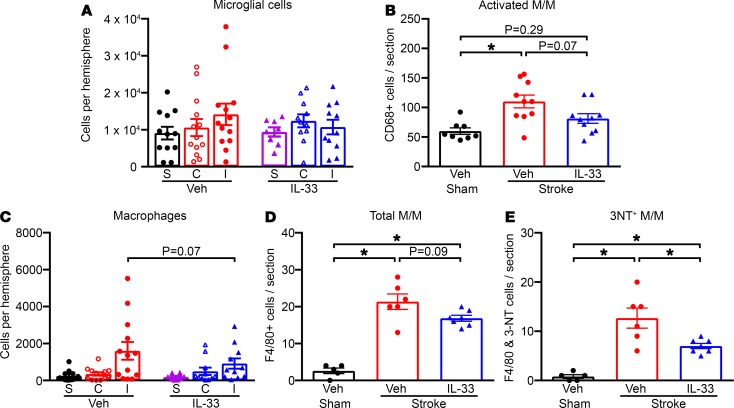
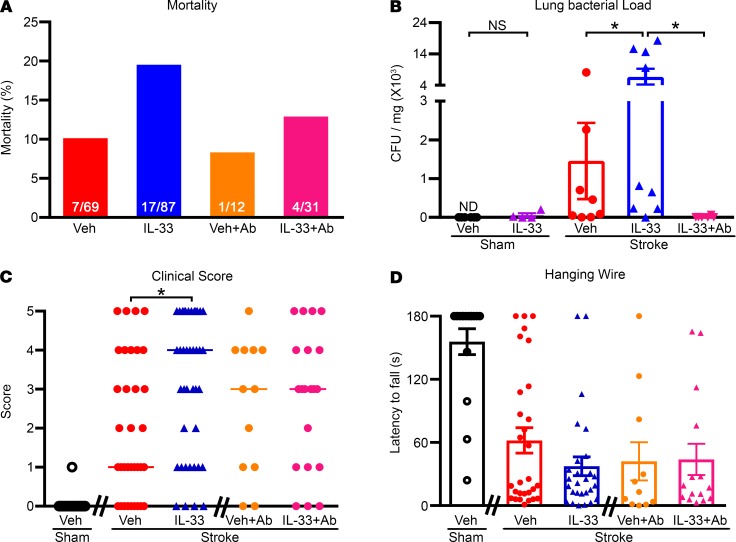
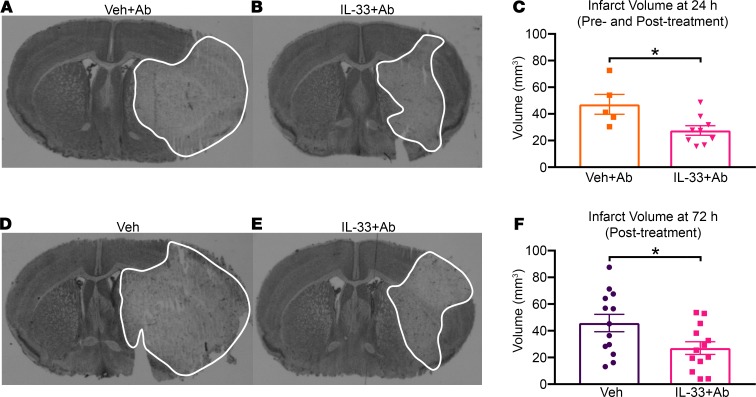
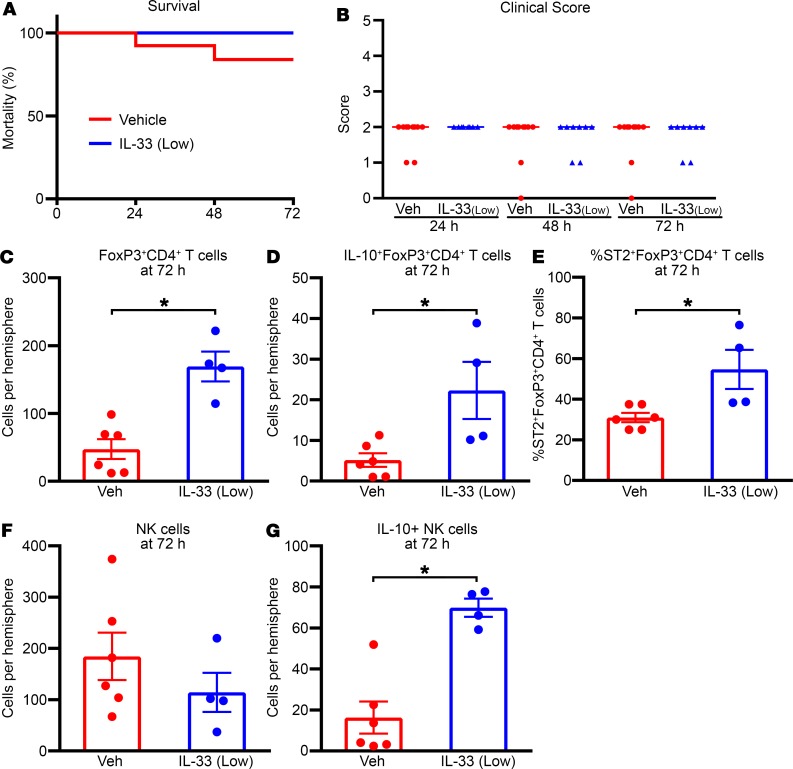
Stroke triggers a complex inflammatory process in which the balance between pro- and antiinflammatory mediators is critical for the development of the brain infarct. However, systemic changes may also occur in parallel with brain inflammation. Here we demonstrate that administration of recombinant IL-33, a recently described member of the IL-1 superfamily of cytokines, promotes Th2-type effects following focal ischemic stroke, resulting in increased plasma levels of Th2-type cytokines and fewer proinflammatory (3-nitrotyrosine+F4/80+) microglia/macrophages in the brain. These effects of IL-33 were associated with reduced infarct size, fewer activated microglia and infiltrating cytotoxic (natural killer-like) T cells, and more IL-10-expressing regulatory T cells. Despite these neuroprotective effects, mice treated with IL-33 displayed exacerbated post-stroke lung bacterial infection in association with greater functional deficits and mortality at 24 hours. Supplementary antibiotics (gentamicin and ampicillin) mitigated these systemic effects of IL-33 after stroke. Our findings highlight the complex nature of the inflammatory mechanisms differentially activated in the brain and periphery during the acute phase after ischemic stroke. The data indicate that a Th2-promoting agent can provide neuroprotection without adverse systemic effects when given in combination with antibiotics.
Keywords: Cardiology; Immunotherapy; Inflammation; Mouse models; Stroke.
Conflict of interest statement
Figures
Similar articles
-
Interleukin-19 alleviates brain injury by anti-inflammatory effects in a mice model of focal cerebral ischemia.Brain Res. 2016 Nov 1;1650:172-177. doi: 10.1016/j.brainres.2016.09.006. Epub 2016 Sep 5. Brain Res. 2016. PMID: 27608956
-
Interleukin-33 Protects Ischemic Brain Injury by Regulating Specific Microglial Activities.Neuroscience. 2018 Aug 10;385:75-89. doi: 10.1016/j.neuroscience.2018.05.047. Epub 2018 Jun 12. Neuroscience. 2018. PMID: 29906552
-
Neuronal Interleukin-4 as a Modulator of Microglial Pathways and Ischemic Brain Damage.J Neurosci. 2015 Aug 12;35(32):11281-91. doi: 10.1523/JNEUROSCI.1685-15.2015. J Neurosci. 2015. PMID: 26269636 Free PMC article.
-
Microglia and Macrophages in Neuroprotection, Neurogenesis, and Emerging Therapies for Stroke.Cells. 2021 Dec 16;10(12):3555. doi: 10.3390/cells10123555. Cells. 2021. PMID: 34944064 Free PMC article. Review.
-
Post-stroke inflammation-target or tool for therapy?Acta Neuropathol. 2019 May;137(5):693-714. doi: 10.1007/s00401-018-1930-z. Epub 2018 Nov 27. Acta Neuropathol. 2019. PMID: 30483945 Free PMC article. Review.
Cited by
-
Therapeutic Opportunities of Interleukin-33 in the Central Nervous System.Front Immunol. 2021 May 17;12:654626. doi: 10.3389/fimmu.2021.654626. eCollection 2021. Front Immunol. 2021. PMID: 34079543 Free PMC article. Review.
-
Immunoreactive Cells After Cerebral Ischemia.Front Immunol. 2019 Nov 26;10:2781. doi: 10.3389/fimmu.2019.02781. eCollection 2019. Front Immunol. 2019. PMID: 31849964 Free PMC article. Review.
-
The immune system and psychiatric disease: a basic science perspective.Clin Exp Immunol. 2019 Sep;197(3):294-307. doi: 10.1111/cei.13334. Epub 2019 Jun 9. Clin Exp Immunol. 2019. PMID: 31125426 Free PMC article. Review.
-
IL-37 increases in patients after ischemic stroke and protects from inflammatory brain injury, motor impairment and lung infection in mice.Sci Rep. 2019 May 6;9(1):6922. doi: 10.1038/s41598-019-43364-7. Sci Rep. 2019. PMID: 31061403 Free PMC article.
-
Soluble Suppression of Tumorigenicity-2 as a Candidate Prognostic Marker for Stroke: A Systematic Review.Ann Lab Med. 2023 Nov 1;43(6):585-595. doi: 10.3343/alm.2023.43.6.585. Epub 2023 Jun 30. Ann Lab Med. 2023. PMID: 37387491 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
