

Extended use of the modified Berlin Definition based on age-related subgroup analysis in pediatric ARDS
- PMID: 30232661
- PMCID: PMC6394569
- DOI: 10.1007/s10354-018-0659-6
Extended use of the modified Berlin Definition based on age-related subgroup analysis in pediatric ARDS
Abstract
Background: Pediatric acute respiratory distress syndrome (pARDS) is a rare but very severe condition. Management of the condition remains a major challenge for pediatric intensive care specialists.
Objective: To perform a descriptive assessment of pARDS based on the modified Berlin Definition by using the SpO2/FiO2 ratio in order to establish an extended patient registry divided into age-related subgroups.
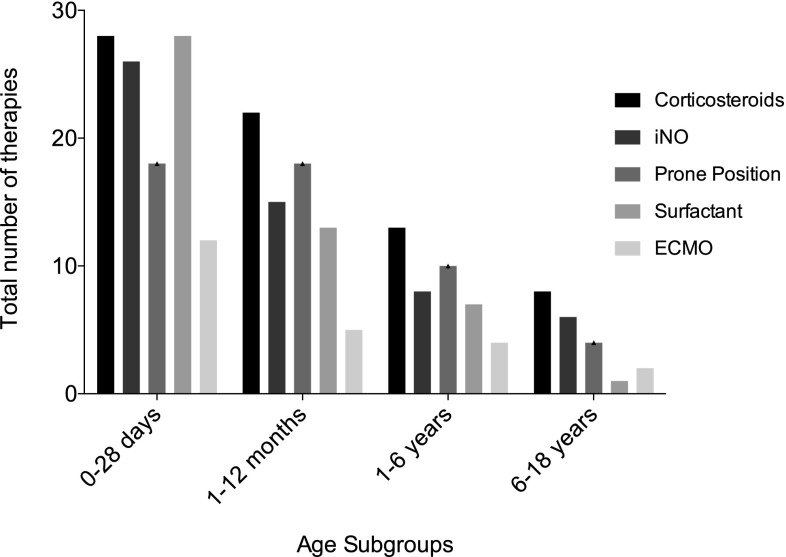
Methods: The data of all children on mechanical ventilation for respiratory failure admitted between 2005 and 2012 were reviewed retrospectively for this study. The age of patients ranged from newborns >37 weeks, up to children <18 years. Inclusion criteria were based on the modified Berlin Definition of pARDS. The following data were collected: demographic data, primary diagnosis, ventilation settings, and use of supportive treatment, in addition to mechanical ventilation (inhaled nitric oxide, surfactant, corticosteroids, prone positioning, and extracorporeal membrane oxygenation).
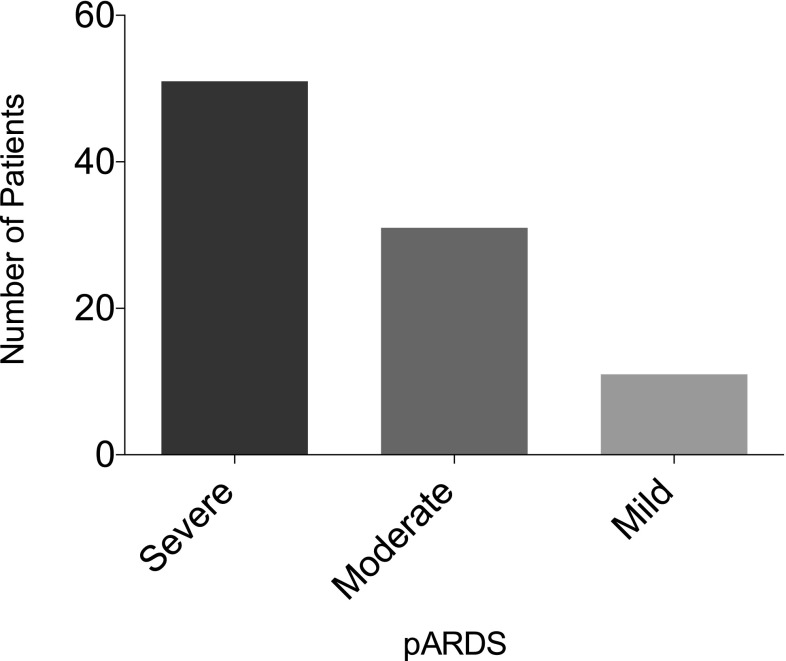
Results: In all, 93 children where included: 35% were newborns, 29% infants, 24% toddlers, and 12% school children; 66% were male and 34% were female patients. The most common primary diagnosis was viral pneumonia (21%) and 55% of the children were diagnosed with severe ARDS. The median duration of stay on the pediatric intensive care unit was 16 days (10/27). In total, 66 children (71%) had direct lung injury and 18 (19%) had indirect lung injury. More than 80% of all children needed more than one supportive care therapy. The overall survival rate was 77%.
Conclusion: This study is a valuable report about pediatric patients with ARDS and allows for an important extension of the application of the modified Berlin Definition in all age groups.
Keywords: ARDS supportive treatment; Berlin Definition; Children; Pediatric ARDS; SpO2/FiO2 ratio.
Conflict of interest statement
Conflict of interest
M. Hermon, S. Dotzler, J.B. Brandt, W. Strohmaier, and J. Golej declare that they have no competing interests and financial potential conflicts do not exist.
Ethical standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments, or comparable ethical standards. For this type of study (retrospective study) informed consent is not required. This study was done with the approval of the of the ethics committee (Medical University of Vienna; Ethic Nr.-1860/2012).
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
