

Spectrum of lytic lesions of the skull: a pictorial essay
- PMID: 30232766
- PMCID: PMC6206388
- DOI: 10.1007/s13244-018-0653-y
Spectrum of lytic lesions of the skull: a pictorial essay
Abstract
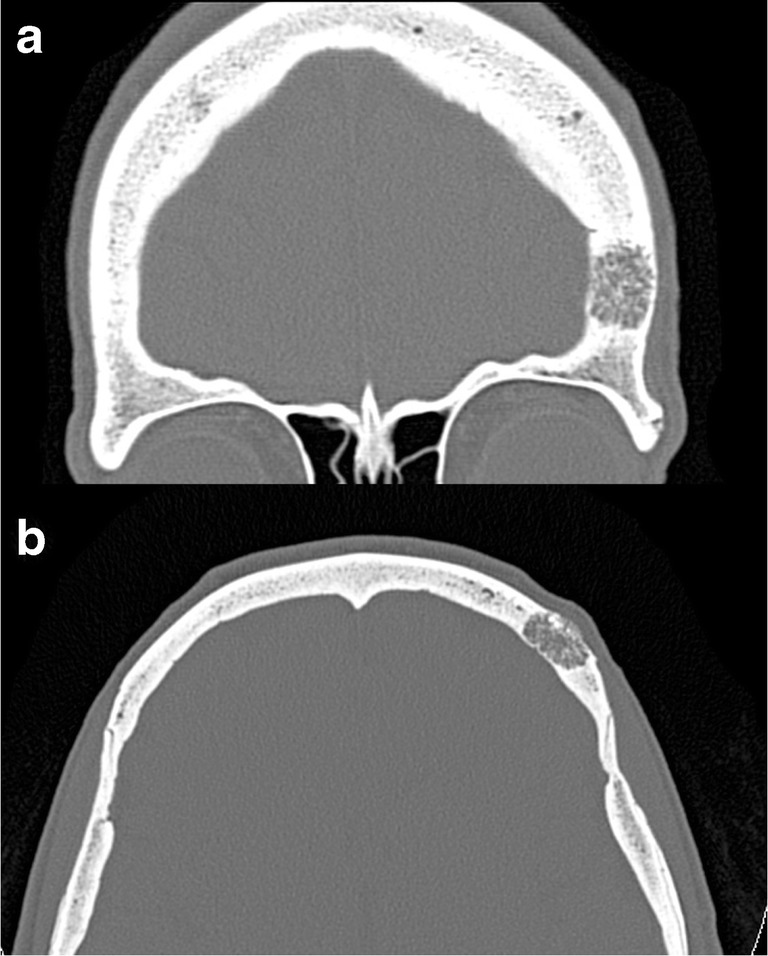
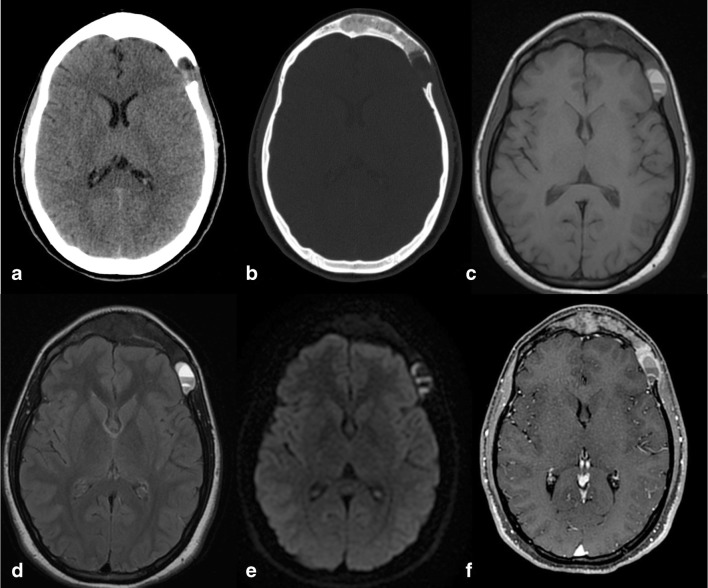
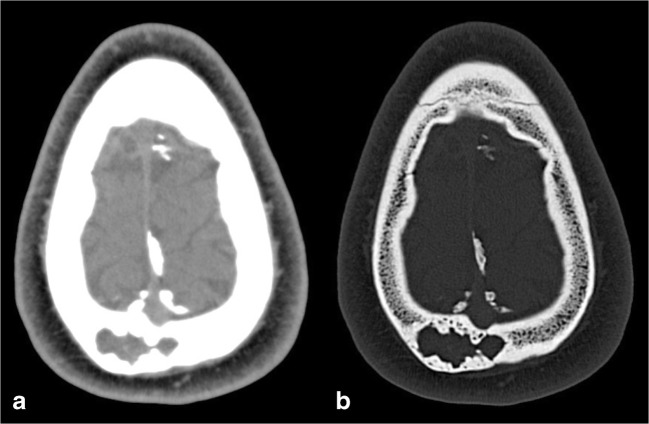
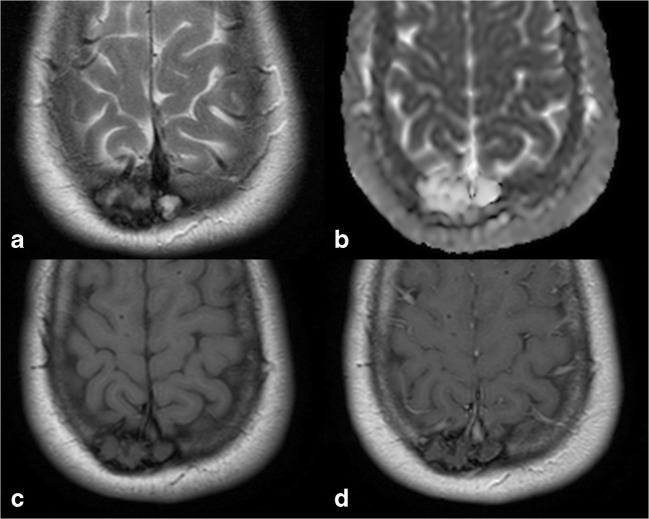
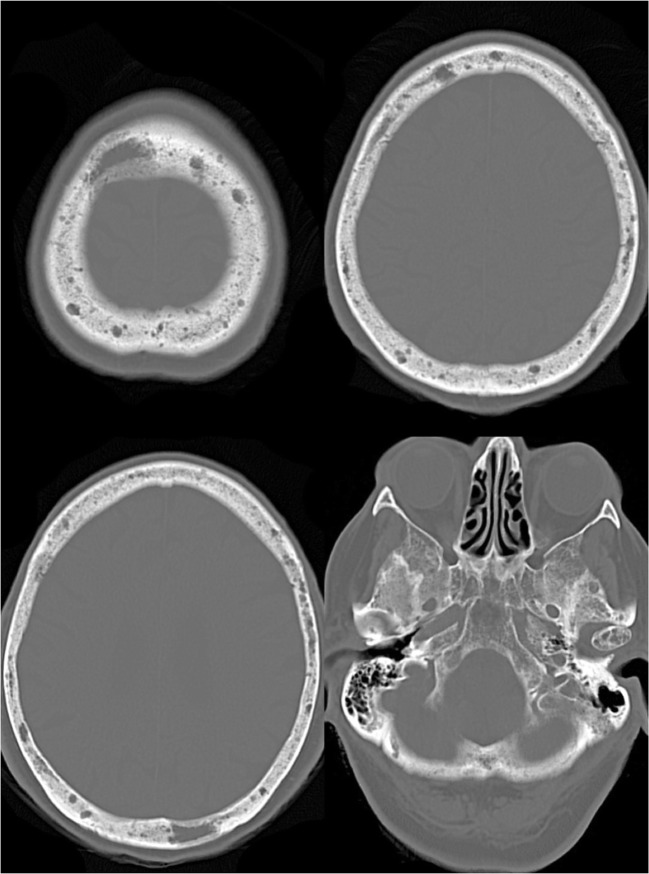
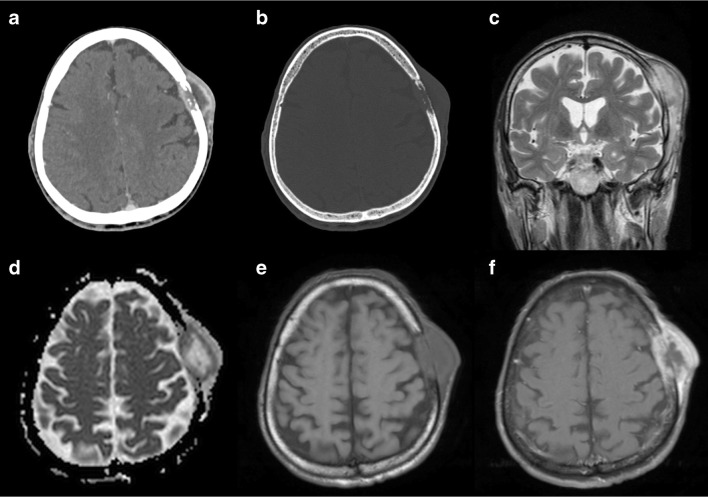
Lytic lesions of the skull include a wide range of diseases, ranging from benign conditions such as arachnoid granulations or vascular lacunae, to aggressive malignant lesions such as lymphomas or metastases. An early and correct characterisation of the nature of the lesion is, therefore, crucial, in order to achieve a fast and appropriate treatment option. In this review, we present the radiological appearance of the most frequent lytic lesions of the skull, describing findings from different imaging modalities (plain X-rays, CT and MRI), with particular attention to diagnostic clues and differential diagnoses. TEACHING POINTS: • Osteolytic skull lesions may be challenging to diagnose. • Association of different imaging techniques may aid image interpretation. • Clinical information and extensive knowledge of possible differential diagnoses is essential. • Some osteolytic tumours, although benign, may present as locally aggressive lesions. • Malignant lesions require accurate staging, followed by variable treatment approaches.
Keywords: Diagnostic imaging; Neoplasms; Radiologists; Review; Skull.
Conflict of interest statement
Conflict of interest
All authors declare no conflict of interest.
Informed consent
Informed consent was previously obtained from all individual participants included in the study.
Ethical approval
For this type of retrospective study, formal consent is not required.
Figures
Similar articles
-
Imaging of pediatric skull lytic lesions: A review.J Neuroimaging. 2024 Jan-Feb;34(1):26-43. doi: 10.1111/jon.13166. Epub 2023 Nov 6. J Neuroimaging. 2024. PMID: 37933199 Review.
-
Radiological review of skull lesions.Insights Imaging. 2018 Oct;9(5):857-882. doi: 10.1007/s13244-018-0643-0. Epub 2018 Sep 19. Insights Imaging. 2018. PMID: 30232767 Free PMC article. Review.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Giant cystic arachnoid granulations: a rare cause of lytic skull lesions.Hum Pathol. 1993 Apr;24(4):438-41. doi: 10.1016/0046-8177(93)90094-w. Hum Pathol. 1993. PMID: 8491484
-
Role of diffusion-weighted imaging in skull base lesions: A pictorial review.Neuroradiol J. 2017 Aug;30(4):370-384. doi: 10.1177/1971400917709624. Epub 2017 Jun 20. Neuroradiol J. 2017. PMID: 28631996 Free PMC article. Review.
Cited by
-
Pediatric orbital lesions: bony and traumatic lesions.Pediatr Radiol. 2024 May;54(6):897-909. doi: 10.1007/s00247-024-05882-z. Epub 2024 Feb 27. Pediatr Radiol. 2024. PMID: 38411665
-
Imaging of skull vault tumors in adults.Insights Imaging. 2020 Feb 13;11(1):23. doi: 10.1186/s13244-019-0820-9. Insights Imaging. 2020. PMID: 32056014 Free PMC article.
-
Metastatic Lung Adenocarcinoma: A Case of Unusual Presentation With a Skull Mass.Cureus. 2023 Jul 24;15(7):e42399. doi: 10.7759/cureus.42399. eCollection 2023 Jul. Cureus. 2023. PMID: 37621819 Free PMC article.
-
Brown Tumour in Chronic Kidney Disease: Revisiting an Old Disease with a New Perspective.Cancers (Basel). 2023 Aug 15;15(16):4107. doi: 10.3390/cancers15164107. Cancers (Basel). 2023. PMID: 37627135 Free PMC article. Review.
-
Aneurysmal bone cyst of the mandible: a rare case report and literature review.Ann Med Surg (Lond). 2023 Aug 8;85(10):5133-5137. doi: 10.1097/MS9.0000000000001168. eCollection 2023 Oct. Ann Med Surg (Lond). 2023. PMID: 37811038 Free PMC article.
References
-
- Arko L, 4th, Berry CT, Desai AS, Weaver M. Intradiploic epidermoid tumors of the cranium: case report with review of the literature. J Neurol Surg A Cent Eur Neurosurg. 2017;78:167–179. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
