

Radiological review of skull lesions
- PMID: 30232767
- PMCID: PMC6206383
- DOI: 10.1007/s13244-018-0643-0
Radiological review of skull lesions
Abstract
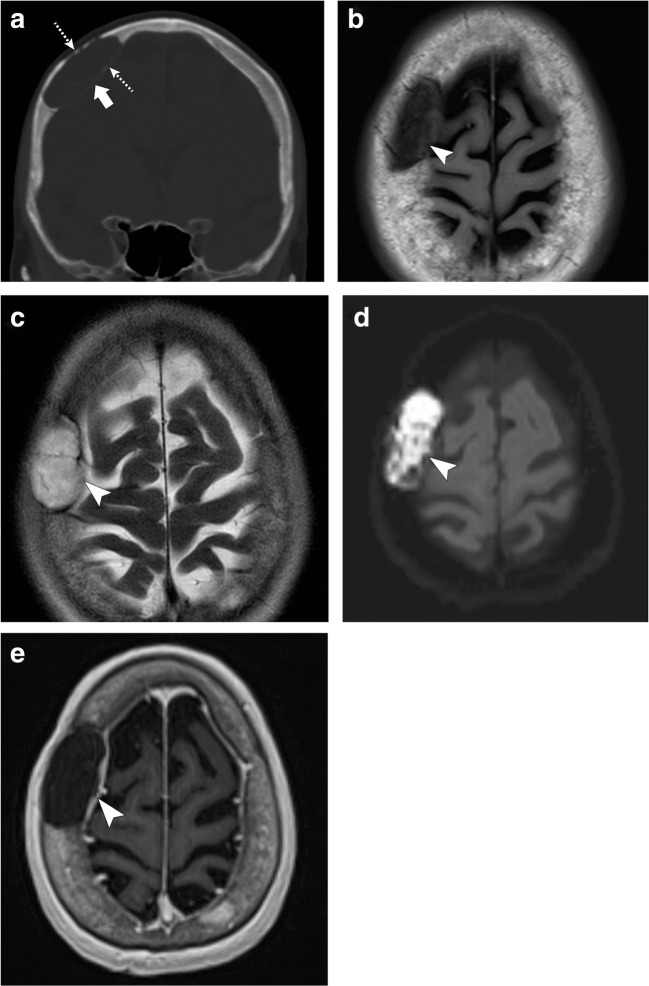
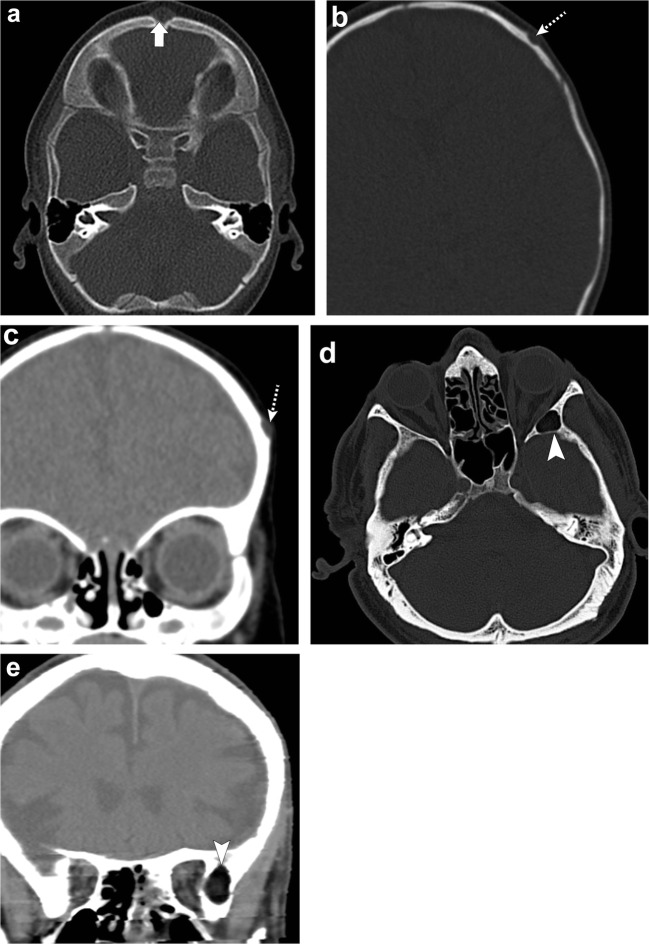
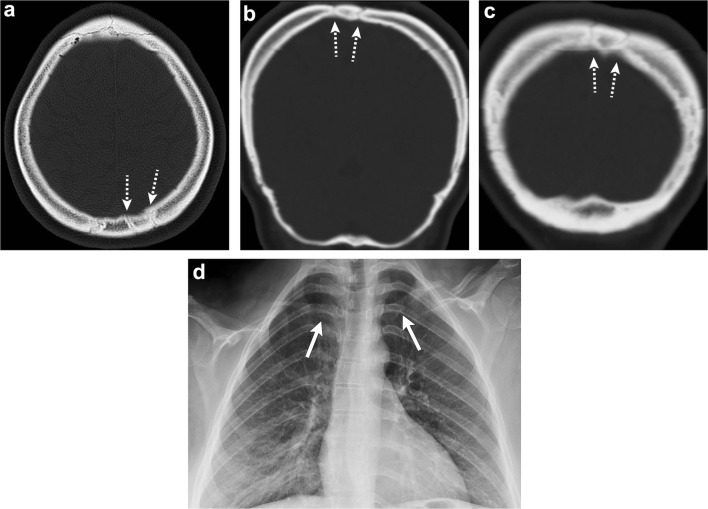
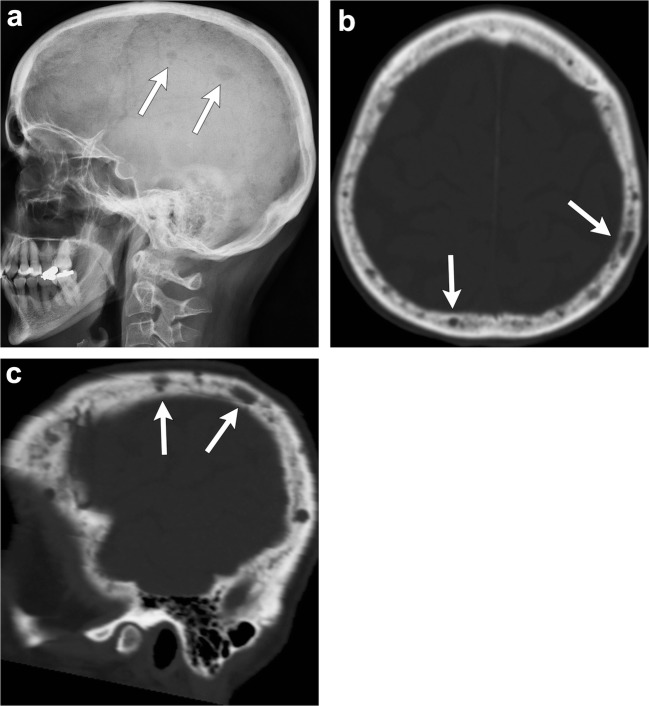
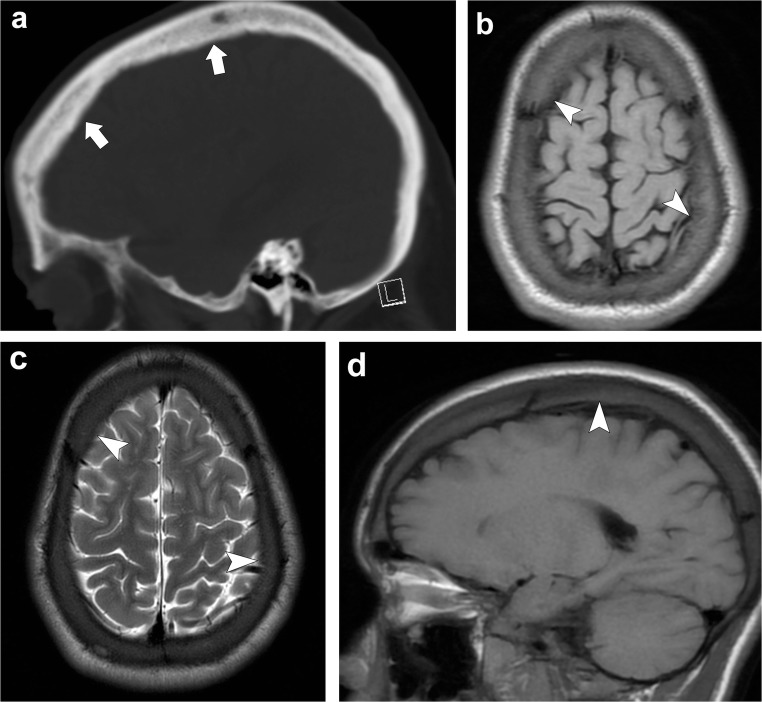
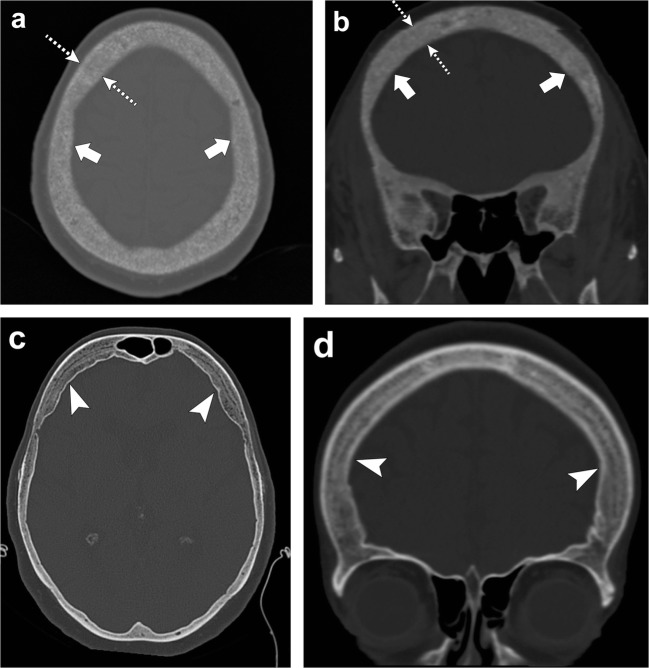
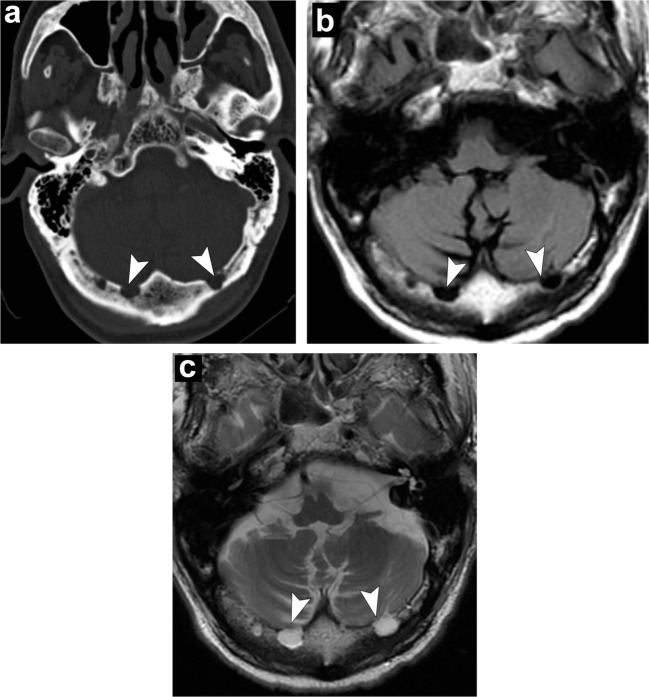
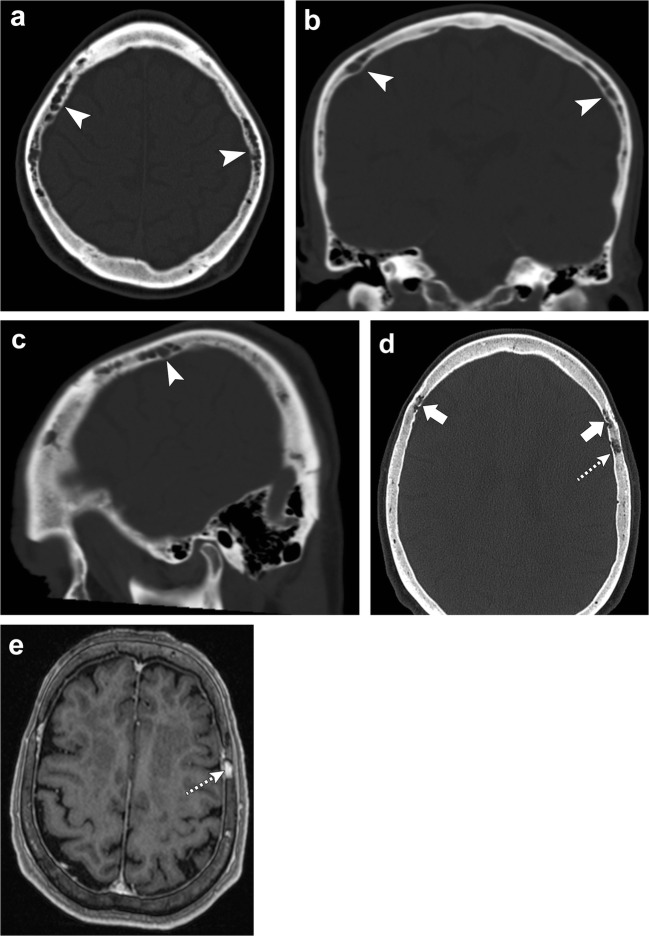
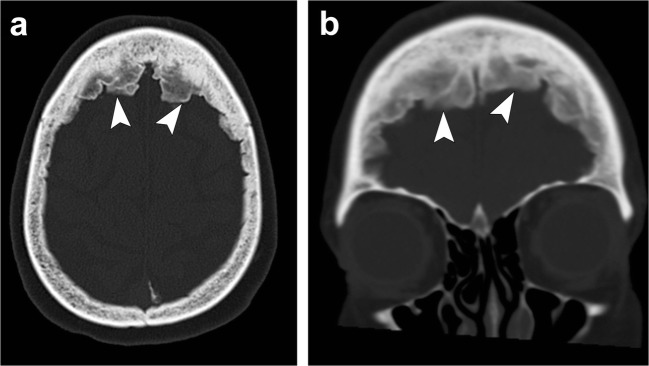
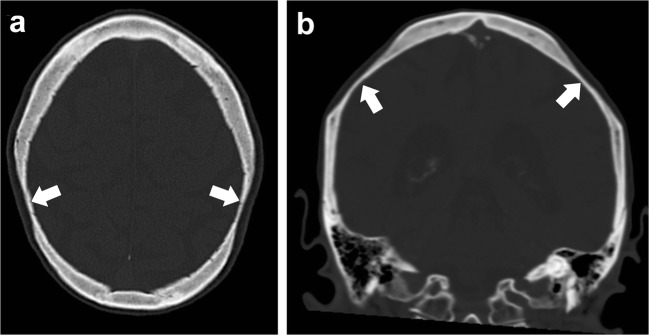
Calvarial lesions are often asymptomatic and are usually discovered incidentally during computed tomography or magnetic resonance imaging of the brain. Calvarial lesions can be benign or malignant. Although the majority of skull lesions are benign, it is important to be familiar with their imaging characteristics and to recognise those with malignant features where more aggressive management is needed. Clinical information such as the age of the patient, as well as the patient's history is fundamental in making the correct diagnosis. In this article, we will review the imaging features of both common and uncommon calvarial lesions, as well as mimics of these lesions found in clinical practice. TEACHING POINTS: • Skull lesions are usually discovered incidentally; they can be benign or malignant. • Metastases are the most frequent cause of skull lesions. • Metastatic lesions are most commonly due to breast cancer in adults and neuroblastoma in children. • Multiple myeloma presents as the classic "punched out" lytic lesions on radiographs. • Eosinophilic granuloma is an osteolytic lesion with bevelled edges.
Keywords: Benign; Calvarial; Lesions; Malignant; Skull.
Conflict of interest statement
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Figures
References
-
- Younghee Y, Woon-Jin M, Hyeong SA, Joon C, Myung HR. Imaging findings of various calvarial bone lesions with a focus on osteolytic lesions. J Korean Soc Radiol. 2016;74(1):43–54. doi: 10.3348/jksr.2016.74.1.43. - DOI
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
