

Total brachial plexus injury: contralateral C7 root transfer to the lower trunk versus the median nerve
- PMID: 30233071
- PMCID: PMC6183026
- DOI: 10.4103/1673-5374.239444
Total brachial plexus injury: contralateral C7 root transfer to the lower trunk versus the median nerve
Abstract
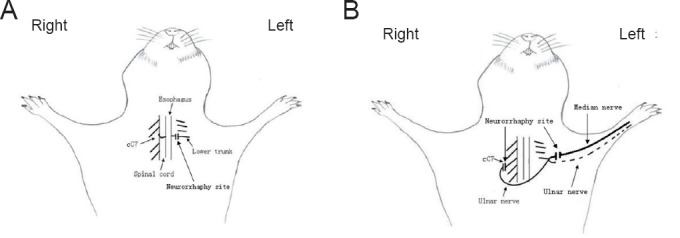
Contralateral C7 (cC7) root transfer to the healthy side is the main method for the treatment of brachial plexus root injury. A relatively new modification of this method involves cC7 root transfer to the lower trunk via the prespinal route. In the current study, we examined the effectiveness of this method using electrophysiological and histological analyses. To this end, we used a rat model of total brachial plexus injury, and cC7 root transfer was performed to either the lower trunk via the prespinal route or the median nerve via a subcutaneous tunnel to repair the injury. At 4, 8 and 12 weeks, the grasping test was used to measure the changes in grasp strength of the injured forepaw. Electrophysiological changes were examined in the flexor digitorum superficialis muscle. The change in the wet weight of the forearm flexor was also measured. Atrophy of the flexor digitorum superficialis muscle was assessed by hematoxylin-eosin staining. Toluidine blue staining was used to count the number of myelinated nerve fibers in the injured nerves. Compared with the traditional method, cC7 root transfer to the lower trunk via the prespinal route increased grasp strength of the injured forepaw, increased the compound muscle action potential maximum amplitude, shortened latency, substantially restored tetanic contraction of the forearm flexor muscles, increased the wet weight of the muscle, reduced atrophy of the flexor digitorum superficialis muscle, and increased the number of myelinated nerve fibers. These findings demonstrate that for finger flexion functional recovery in rats with total brachial plexus injury, transfer of the cC7 root to the lower trunk via the prespinal route is more effective than transfer to the median nerve via subcutaneous tunnel.
Keywords: contralateral C7 root; lower trunk; median nerve; nerve regeneration; nerve transfer; neural regeneration; total brachial plexus injury.
Conflict of interest statement
The authors declare that they have no conflicts of interest
Figures


Similar articles
-
Contralateral C7 transfer to lower trunk via the prespinal route in the repair of brachial plexus injury: an experimental study in rats.J Plast Reconstr Aesthet Surg. 2014 Sep;67(9):1282-7. doi: 10.1016/j.bjps.2014.05.024. Epub 2014 Jun 2. J Plast Reconstr Aesthet Surg. 2014. PMID: 24951029
-
Comparative study of intercostal nerve transfer to lower trunk and contralateral C7 root transfer in repair of total brachial plexus injury in rats.J Plast Reconstr Aesthet Surg. 2016 May;69(5):623-8. doi: 10.1016/j.bjps.2015.11.004. Epub 2015 Nov 25. J Plast Reconstr Aesthet Surg. 2016. PMID: 26702947
-
Contralateral C7 nerve transfer with direct coaptation to restore lower trunk function after traumatic brachial plexus avulsion.J Bone Joint Surg Am. 2013 May 1;95(9):821-7, S1-2. doi: 10.2106/JBJS.L.00039. J Bone Joint Surg Am. 2013. PMID: 23636189
-
An electroencephalography-based human-machine interface combined with contralateral C7 transfer in the treatment of brachial plexus injury.Neural Regen Res. 2022 Dec;17(12):2600-2605. doi: 10.4103/1673-5374.335838. Neural Regen Res. 2022. PMID: 35662188 Free PMC article. Review.
-
A systematic review of outcomes of contralateral C-7 transfer for the treatment of traumatic brachial plexus injury: an international comparison.J Neurosurg. 2017 Mar;126(3):922-932. doi: 10.3171/2016.1.JNS152597. Epub 2016 Apr 29. J Neurosurg. 2017. PMID: 27128594
Cited by
-
Functional outcome of contralateral C7 nerve transfer combined with free functional gracilis transplantation to repair total brachial plexus avulsion: a report of thirty-nine cases.Int Orthop. 2022 May;46(5):1053-1062. doi: 10.1007/s00264-021-05108-z. Epub 2022 Feb 3. Int Orthop. 2022. PMID: 35113187 Free PMC article.
-
Melatonin combined with chondroitin sulfate ABC promotes nerve regeneration after root-avulsion brachial plexus injury.Neural Regen Res. 2019 Feb;14(2):328-338. doi: 10.4103/1673-5374.244796. Neural Regen Res. 2019. PMID: 30531017 Free PMC article.
-
Comparison between direct repair and human acellular nerve allografting during contralateral C7 transfer to the upper trunk for restoration of shoulder abduction and elbow flexion.Neural Regen Res. 2019 Dec;14(12):2132-2140. doi: 10.4103/1673-5374.262600. Neural Regen Res. 2019. PMID: 31397352 Free PMC article.
-
A bibliometric analysis of brachial plexus injury from 1980 to 2022.Heliyon. 2024 Feb 16;10(4):e26175. doi: 10.1016/j.heliyon.2024.e26175. eCollection 2024 Feb 29. Heliyon. 2024. PMID: 38434026 Free PMC article. Review.
-
Effects of Akt/mTOR/p70S6K Signaling Pathway Regulation on Neuron Remodeling Caused by Translocation Repair.Front Neurosci. 2020 Sep 29;14:565870. doi: 10.3389/fnins.2020.565870. eCollection 2020. Front Neurosci. 2020. PMID: 33132828 Free PMC article.
References
-
- Bentolila V, Nizard R, Bizot P, Sedel L. Complete traumatic brachial plexus palsy. Treatment and outcome after repair. J Bone Joint Surg Am. 1999;81:20–28. - PubMed
-
- Bertelli JA, Ghizoni MF. Transfer of a flexor digitorum superficialis motor branch for wrist extension reconstruction in C5-C8 root injuries of the brachial plexus: a case series. Microsurgery. 2013;33:39–42. - PubMed
-
- Brunelli G, Monini L. Neurotization of avulsed roots of brachial plexus by means of anterior nerves of cervical plexus. Clin Plast Surg. 1984;11:149–152. - PubMed
-
- Chuang DC. Neurotization procedures for brachial plexus injuries. Hand Clin. 1995;11:633–645. - PubMed
-
- Chuang DC, Hernon C. Minimum 4-year follow-up on contralateral C7 nerve transfers for brachial plexus injuries. J Hand Surg Am. 2012;37:270–276. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
