

Total brachial plexus injury: contralateral C7 root transfer to the lower trunk versus the median nerve
- PMID: 30233071
- PMCID: PMC6183026
- DOI: 10.4103/1673-5374.239444
Total brachial plexus injury: contralateral C7 root transfer to the lower trunk versus the median nerve
Abstract
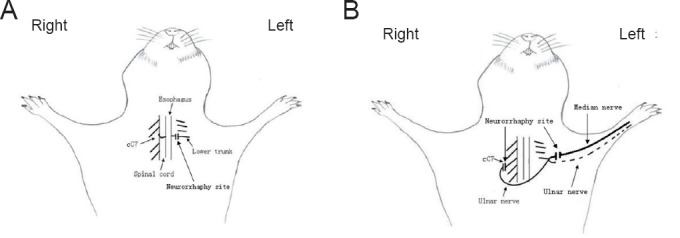
Contralateral C7 (cC7) root transfer to the healthy side is the main method for the treatment of brachial plexus root injury. A relatively new modification of this method involves cC7 root transfer to the lower trunk via the prespinal route. In the current study, we examined the effectiveness of this method using electrophysiological and histological analyses. To this end, we used a rat model of total brachial plexus injury, and cC7 root transfer was performed to either the lower trunk via the prespinal route or the median nerve via a subcutaneous tunnel to repair the injury. At 4, 8 and 12 weeks, the grasping test was used to measure the changes in grasp strength of the injured forepaw. Electrophysiological changes were examined in the flexor digitorum superficialis muscle. The change in the wet weight of the forearm flexor was also measured. Atrophy of the flexor digitorum superficialis muscle was assessed by hematoxylin-eosin staining. Toluidine blue staining was used to count the number of myelinated nerve fibers in the injured nerves. Compared with the traditional method, cC7 root transfer to the lower trunk via the prespinal route increased grasp strength of the injured forepaw, increased the compound muscle action potential maximum amplitude, shortened latency, substantially restored tetanic contraction of the forearm flexor muscles, increased the wet weight of the muscle, reduced atrophy of the flexor digitorum superficialis muscle, and increased the number of myelinated nerve fibers. These findings demonstrate that for finger flexion functional recovery in rats with total brachial plexus injury, transfer of the cC7 root to the lower trunk via the prespinal route is more effective than transfer to the median nerve via subcutaneous tunnel.
Keywords: contralateral C7 root; lower trunk; median nerve; nerve regeneration; nerve transfer; neural regeneration; total brachial plexus injury.
Conflict of interest statement
The authors declare that they have no conflicts of interest
Figures


References
-
- Bentolila V, Nizard R, Bizot P, Sedel L. Complete traumatic brachial plexus palsy. Treatment and outcome after repair. J Bone Joint Surg Am. 1999;81:20–28. - PubMed
-
- Bertelli JA, Ghizoni MF. Transfer of a flexor digitorum superficialis motor branch for wrist extension reconstruction in C5-C8 root injuries of the brachial plexus: a case series. Microsurgery. 2013;33:39–42. - PubMed
-
- Brunelli G, Monini L. Neurotization of avulsed roots of brachial plexus by means of anterior nerves of cervical plexus. Clin Plast Surg. 1984;11:149–152. - PubMed
-
- Chuang DC. Neurotization procedures for brachial plexus injuries. Hand Clin. 1995;11:633–645. - PubMed
-
- Chuang DC, Hernon C. Minimum 4-year follow-up on contralateral C7 nerve transfers for brachial plexus injuries. J Hand Surg Am. 2012;37:270–276. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
