

A Novel Scoring System for Rupture Risk Stratification of Intracranial Aneurysms: A Hemodynamic and Morphological Study
- PMID: 30233292
- PMCID: PMC6133991
- DOI: 10.3389/fnins.2018.00596
A Novel Scoring System for Rupture Risk Stratification of Intracranial Aneurysms: A Hemodynamic and Morphological Study
Abstract
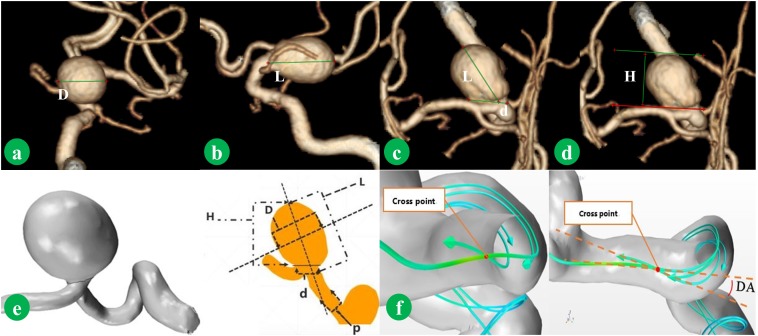
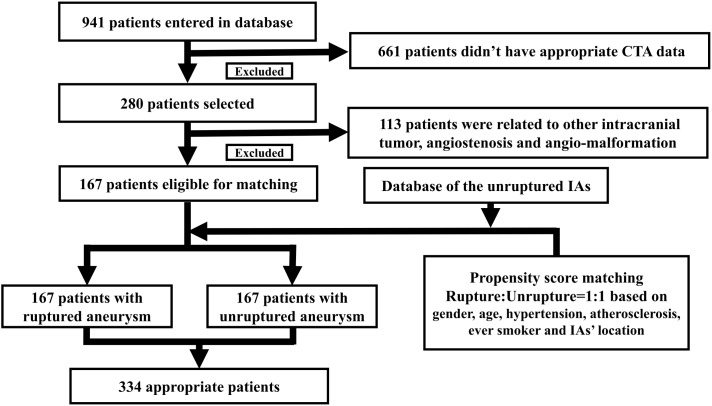
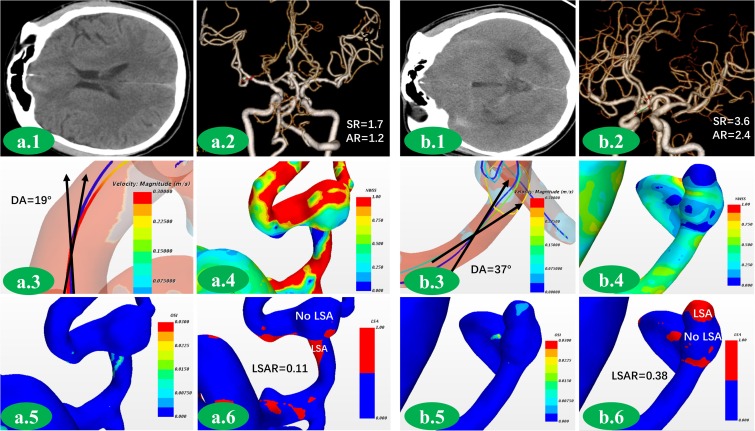
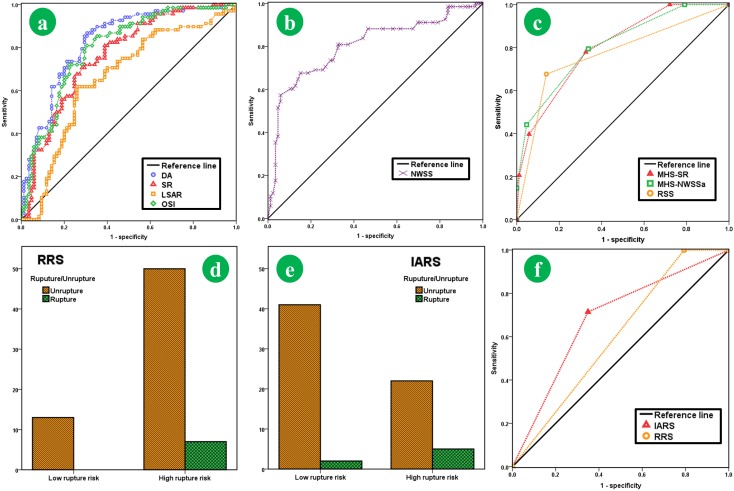
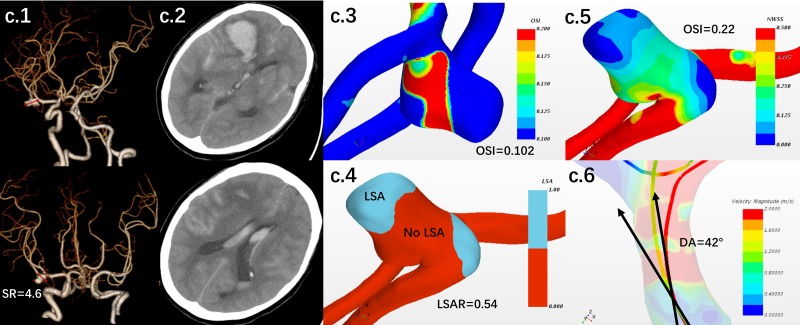
Objective: The aim of the present study is to investigate the potential morphological and hemodynamic risk factors related to intracranial aneurysms (IAs) rupture and establish a system to stratify the risk of IAs rupture to help the clinical decision-making. Methods: Patients admitted to our hospital for single-IAs were selected from January 2012 and January 2018. A propensity score matching was conducted to match patients. The morphological parameters were obtained from high solution CTA images, and the hemodynamic parameters were obtained in accordance with the outcomes of computational fluid dynamics (CFDs) simulation. Differences in the morphologic and hemodynamic parameters were compared. The significant parameters were selected to establish a novel scoring system (Intracranial Aneurysm Rupture Score, IARS). The comparison was drawn between the discriminating accuracy of IARS and the Rupture Resemblance Score (RRS) system to verify the value of IARS. Then, a group of patients with unruptured IAs was stratified into the high risk and low risk groups by IARS and RRS system separately and was followed up for 18-27 months to verify the value of IARS. The outcome of different stratifications was compared. Results: The matching process yielded 167 patients in each group. Differences of statistical significance were found in aneurysm length (p = 0.001), perpendicular height (H) (p < 0.001), aspect ratio (AR) (p < 0.001), size ratio (SR) (p < 0.001), deviated angle (DA) (p < 0.001), normalized average wall shear stress (NWSSa) (p < 0.001), wall shear stress gradient (WSSG) (p < 0.001), low shear area ratio (LSAR) (p = 0.01), and oscillatory shear index (OSI) (p = 0.01). Logistic regression analysis further demonstrated that SR, DA, NWSSa, LSAR, and OSI were the independent risk factors of IAs rupture. SR, DA, LSAR, and OSI were finally selected to establish the IARS. Our present IARS showed a higher discriminating value (AUC 0.81 vs. 0.77) in comparison with the RRS (SR, NWSSa, and OSI). After follow-up, seven patients were subject to IAs rupture. 5/26 in high risk group stratified by IARS, yet 7/57 in high risk group stratified by RRS. The accuracy of IARS was further verified (19.2% vs. 12.3%, AUC for the IARS and the RRS was 0.723 and 0.673, respectively). Conclusion: SR, DA, NWSSa, LSAR, and OSI were considered the independent risk factors of IAs rupture. Our novel IARS showed higher accuracy in discriminating IA rupture in comparison with RRS.
Keywords: computational fluid dynamics; hemodynamic; intracranial aneurysm; morphological; rupture.
Figures
References
-
- Chen C. J., Moosa S., Ding D., Raper D. M., Burke R. M., Lee C. C., et al. (2016). Infundibular dilations of the posterior communicating arteries: pathogenesis, anatomical variants, aneurysm formation, and subarachnoid hemorrhage. J. Neurointerv. Surg. 8 791–795. 10.1136/neurintsurg-2015-011827 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials