

Magnetic resonance imaging findings in ovarian torsion post in vitro fertilization
- PMID: 30233749
- PMCID: PMC6138859
- DOI: 10.1016/j.radcr.2018.08.003
Magnetic resonance imaging findings in ovarian torsion post in vitro fertilization
Abstract
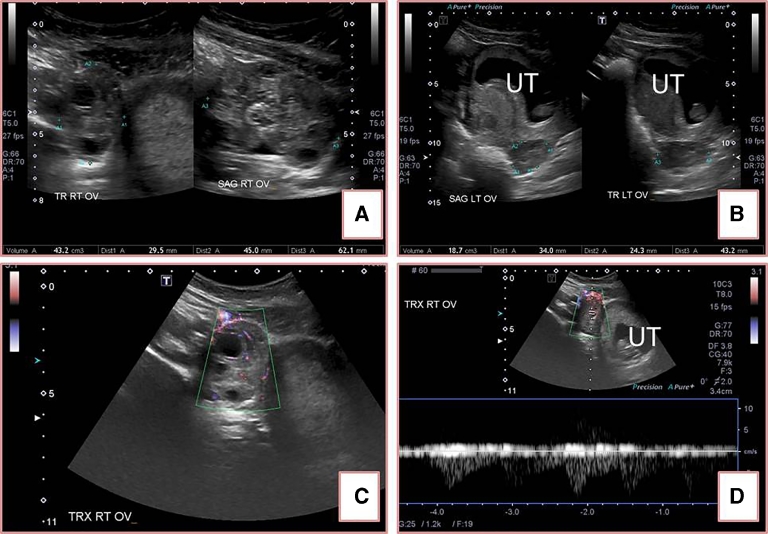
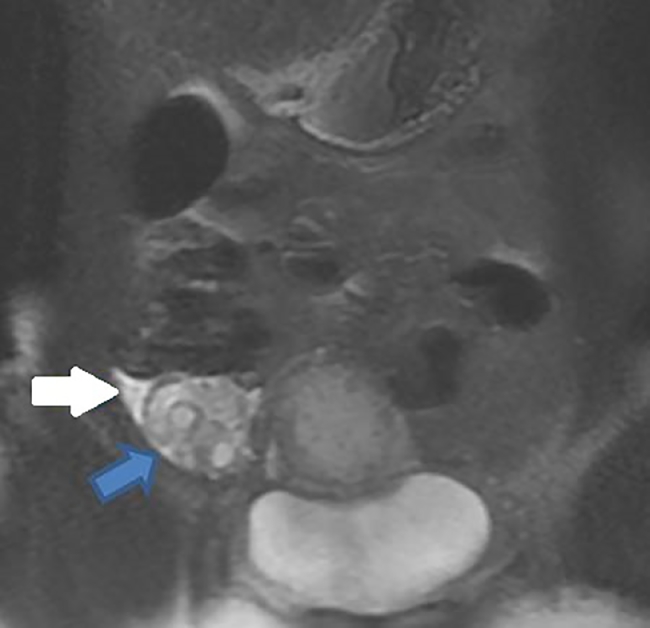
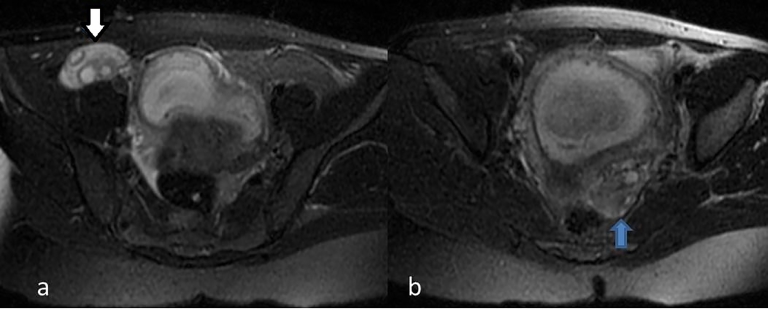
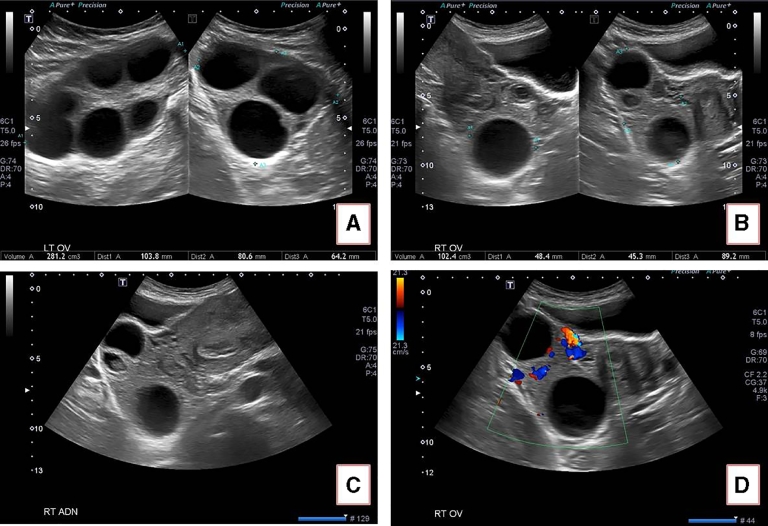
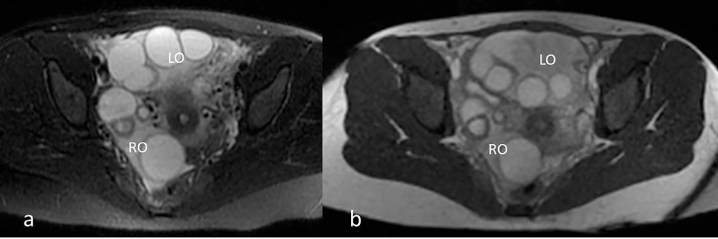
Patients who get pregnant after being treated with in vitro fertilization (IVF) are at significantly increased risk of ovarian torsion compared to the general population and also in comparison to patients who get pregnant normally [1,2]. The risk is further increased in patients who develop ovarian hyperstimulation syndrome [1]. This possibility should be considered in this group of patients presenting with acute abdominal pain and immediate management should be commenced. Here, we report 2 patients who received treatment for infertility with IVF and developed ovarian torsion and we discuss their management including the imaging workup. The first case is a 34-year-old woman at 11 + 3 weeks of gestation after IVF who presented with a 12-hour acute right lower abdominal pain with nausea and vomiting. She underwent an ultrasound examination and then further evaluated with magnetic resonance imaging which showed asymmetric enlargement of the right ovary and stromal edema and a diagnosis of ovarian torsion was made. The patient underwent laparoscopic detortion and the ovary was salvaged. The second case is a 33-year-old woman at 9 weeks of gestation after IVF who presented with intermittent abdominal pain, vaginal bleeding, and nausea and vomiting for 5 days but became worse on the fifth day. Ultrasound and subsequently magnetic resonance imaging were performed which confirmed hyperstimulation syndrome. Abnormal location of the left ovary anterior to the uterus with higher volume as well as the clinical progression raised the possibility of ovarian torsion and prompted a diagnostic laparoscopy which showed right ovarian torsion and detortion was performed.
Keywords: Complication; In vitro fertilization; Ovarian torsion; Pregnancy.
Figures
Similar articles
-
Acute abdomen in early pregnancy due to ovarian torsion following successful in vitro fertilization treatment.Taiwan J Obstet Gynecol. 2015 Aug;54(4):438-41. doi: 10.1016/j.tjog.2013.08.013. Taiwan J Obstet Gynecol. 2015. PMID: 26384066
-
Laparoscopic detorsion of the ovary in ovarian hyperstimulation syndrome during the sixth week of gestation: A case report and review.Int J Surg Case Rep. 2019;59:50-53. doi: 10.1016/j.ijscr.2019.04.051. Epub 2019 May 9. Int J Surg Case Rep. 2019. PMID: 31103953 Free PMC article.
-
Ovarian torsion in in vitro fertilization-induced twin pregnancy: combination of Doppler ultrasound and laparoscopy in diagnosis and treatment can quickly solve the case.Fertil Steril. 2009 Oct;92(4):1496.e9-1496.e13. doi: 10.1016/j.fertnstert.2009.06.029. Epub 2009 Jul 24. Fertil Steril. 2009. PMID: 19631937
-
Adnexal torsion in pregnancy after in vitro fertilization: Case report and literature review.Medicine (Baltimore). 2021 Jan 22;100(3):e24009. doi: 10.1097/MD.0000000000024009. Medicine (Baltimore). 2021. PMID: 33545996 Free PMC article. Review.
-
Successful pregnancy complicated by early and late adnexal torsion after in vitro fertilization.Fertil Steril. 2007 Mar;87(3):697.e9-12. doi: 10.1016/j.fertnstert.2006.05.091. Epub 2006 Dec 4. Fertil Steril. 2007. PMID: 17141765 Review.
References
-
- Damigos E, Johns J, Ross J. An update on the diagnosis and management of ovarian torsion. Obstet Gynaecol. 2012;14:229–236.
-
- Johnson TR, Jr, Woodruff JD. Surgical emergencies of the uterine adnexae during pregnancy. Int J Gynaecol Obstet. 1986;24:331–335. - PubMed
-
- Hibbard LT. Adnexal torsion. Am J Obstet Gynecol. 1985;152:456–461. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
