

Does age over 80 years have to be a contraindication for lung cancer surgery-a nationwide database study
- PMID: 30233848
- PMCID: PMC6129874
- DOI: 10.21037/jtd.2018.07.12
Does age over 80 years have to be a contraindication for lung cancer surgery-a nationwide database study
Abstract
Background: Nowadays surgery remains the best treatment for localized lung cancer (LC). However, patients over 80 years old are often denied surgery because of the postoperative risk of death. This study aimed to estimate in-hospital mortality (IHM) and determine whether age over 80 is the most important predictor of IHM after LC surgery.
Methods: From January 2005 to December 2015, 97,440 patients, including 4,438 patients over 80 years old, were operated on for LC and recorded in the French Administrative Database. Characteristics of patients, hospitals and surgery were analysed.
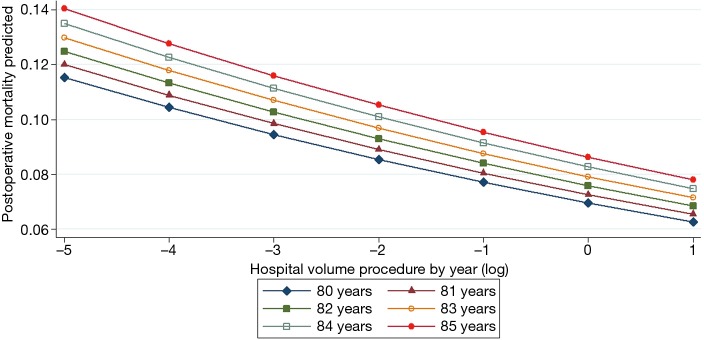
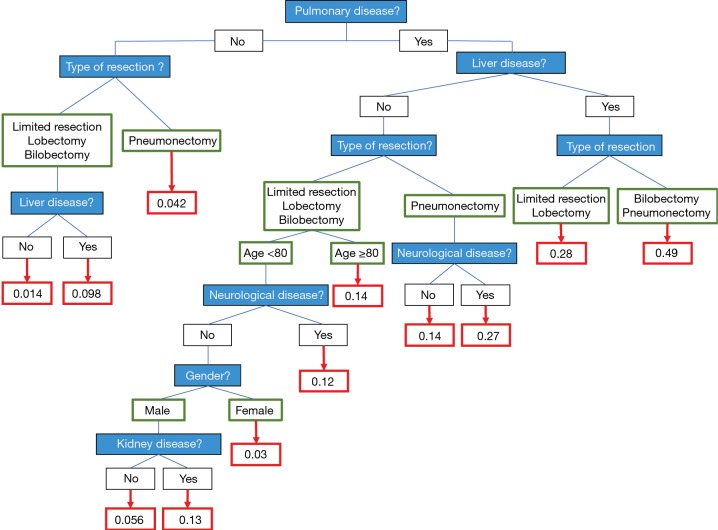
Results: Crude IHM was 3.73% (n=3,639) and 7.77% (n=345) for the over 80s vs. 3.54% (n=3,294) for younger patients (P<0.0001). In multivariate analysis, predictive factors for IHM with the odds ratios (OR) were: 2.60 for age ≥80 (95% CI: 2.30-2.94; P=0.0001), 5.85 for a previous liver disease (95% CI: 4.79-7.16; P=0.0001) and 5 for previous lung disease (95% CI: 4.25-5.9; P=0.0001). IHM was also linked to hospital volume with an OR of 0.75 (95% CI: 0.69-0.81; P=0.0001) and a linear decrease for predicted IHM according to hospital volume for the over 80s. Adjusted ORs were 1.15 (95% CI: 0.96-1.4; P=0.0116) for lobectomy, 2.18 for bilobectomy (95% CI: 1.7-2.8; P=0.0001) and 3.83 (95% CI: 3.2-4.6; P=0.0001) for pneumonectomy.
Conclusions: Concerning IHM, age ≥80 had a lower weight than did a previous pulmonary or liver disease and the type of pulmonary resection. Patients over 80s with localized LC and no significant comorbidities should be referred for surgery if lobectomy or sublobar resection could be performed.
Keywords: Over 80s; in-hospital mortality (IHM); lobectomy; nationwide database; predictive factors.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
-
- Social Security Administration 2010. Available online: http://www.ssa.gov/OACT/STATS/table4c6.html
-
- United Nations Department of Economic and Social Affairs population Division. World population ageing: 1950e2050. Available online: http://www.un.org/esa/population/publications/worldageing19502050
-
- Howington JA, Blum MG, Chang AC, et al. Treatment of stage I and II non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e278S-313S. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources