

Comparison of different methods of postoperative analgesia after thoracotomy-a randomized controlled trial
- PMID: 30233861
- PMCID: PMC6129891
- DOI: 10.21037/jtd.2018.07.88
Comparison of different methods of postoperative analgesia after thoracotomy-a randomized controlled trial
Abstract
Background: Continuous thoracic epidural analgesia (TEA) is a preferred method of postoperative analgesia in thoracic surgery. Intravenous patient-controlled analgesia (IVPCA) may be an effective alternative. One of the most commonly used opioids in PCA is morphine. It has high antinociceptive efficacy but is associated with many adverse events. Oxycodone can be an alternative. A small number of scientific reports comparing morphine and oxycodone in PCA for the treatment of acute postoperative pain after thoracotomy was the reason to conduct this study.
Methods: Prospective, randomised, observational study. In total of 99 patients scheduled for elective thoracotomy were randomized into three study groups. TEA group received continuous TEA as a method of postoperative pain management, morphine (MF) group received morphine IVPCA, and morphine (OXY) group oxycodone IVPCA. For 48 hours' hemodynamic parameters, level of pain, sedation and the need for rescue analgesia were monitored. After 48 hours' patients were asked about their satisfaction with pain treatment using Likert scale and assessment of opioid related adverse events via overall benefit of analgesia score (OBAS).
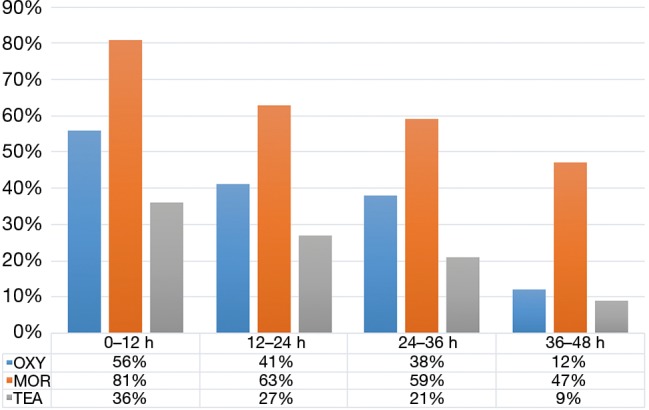
Results: The level of pain in visual analogic score (VAS) and Prince Henry Hospital Pain Score (PHHPS) scales was significantly lower in TEA group with no significant difference between groups MF and OXY. Using morphine in PCA was associated with a significantly higher likelihood of need of rescue analgesia. The level of sedation in Ramsay scale was significantly higher in MF compared to OXY and TEA group. There were no significant differences between groups in OBAS scale. TEA group was characterized by the highest degree of patient satisfaction.
Conclusions: TEA provided superior anaesthesia compared to PCA in our study group. Use of PCA oxycodone in postoperative pain management after open thoracotomy provides similar nociception control compared to morphine but is associated with less sedation and patients using oxycodone IVPCA require smaller doses of rescue analgesia compared to systemic morphine IVPCA.
Keywords: Postoperative analgesia; morphine; oxycodone; patient-controlled analgesia (PCA); thoracotomy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical