

Evaluation of Haptic Feedback on Bimanually Teleoperated Laparoscopy for Endometriosis Surgery
- PMID: 30235114
- PMCID: PMC6488009
- DOI: 10.1109/TBME.2018.2870542
Evaluation of Haptic Feedback on Bimanually Teleoperated Laparoscopy for Endometriosis Surgery
Abstract
Robotic minimal invasive surgery is gaining acceptance in surgical care. In contrast with the appreciated three-dimensional vision and enhanced dexterity, haptic feedback is not offered. For this reason, robotics is not considered beneficial for delicate interventions such as the endometriosis. Overall, haptic feedback remains debatable and yet unproven except for some simple scenarios such as fundamentals of laparoscopic surgery exercises.
Objective: This work investigates the benefits of haptic feedback on more complex surgical gestures, manipulating delicate tissue through coordination between multiple instruments.
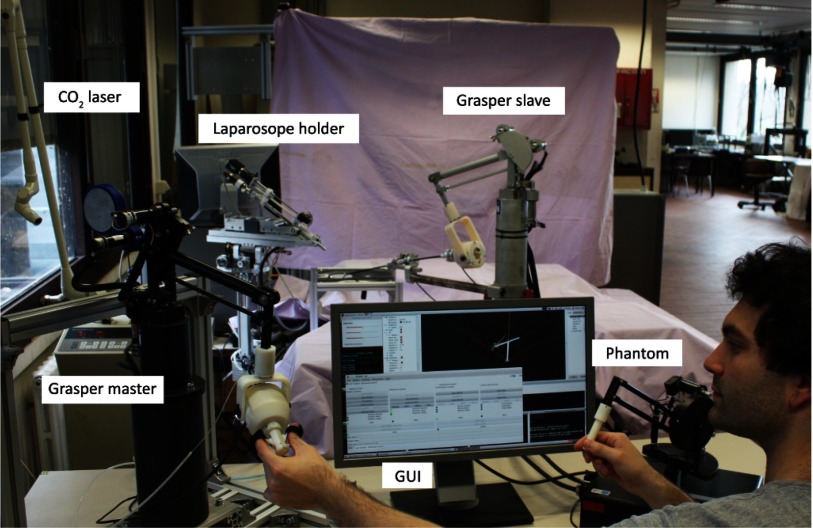
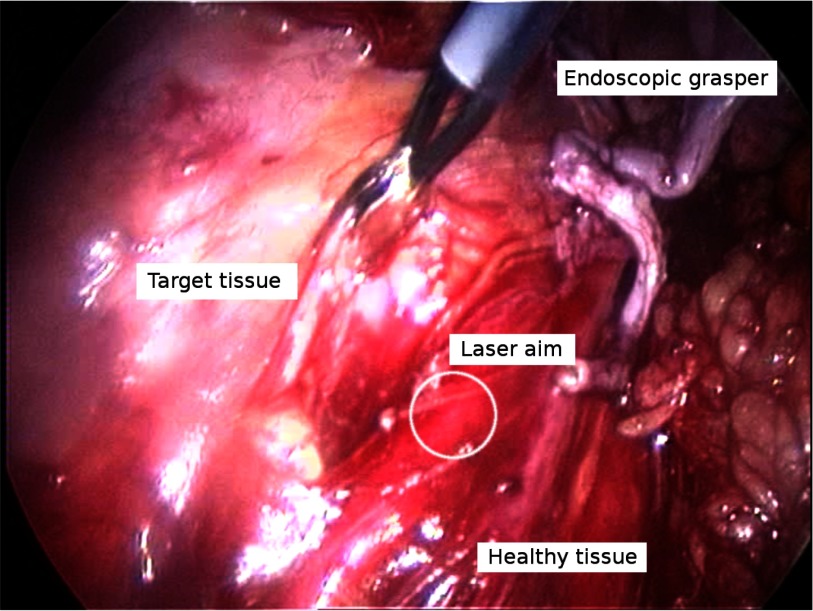
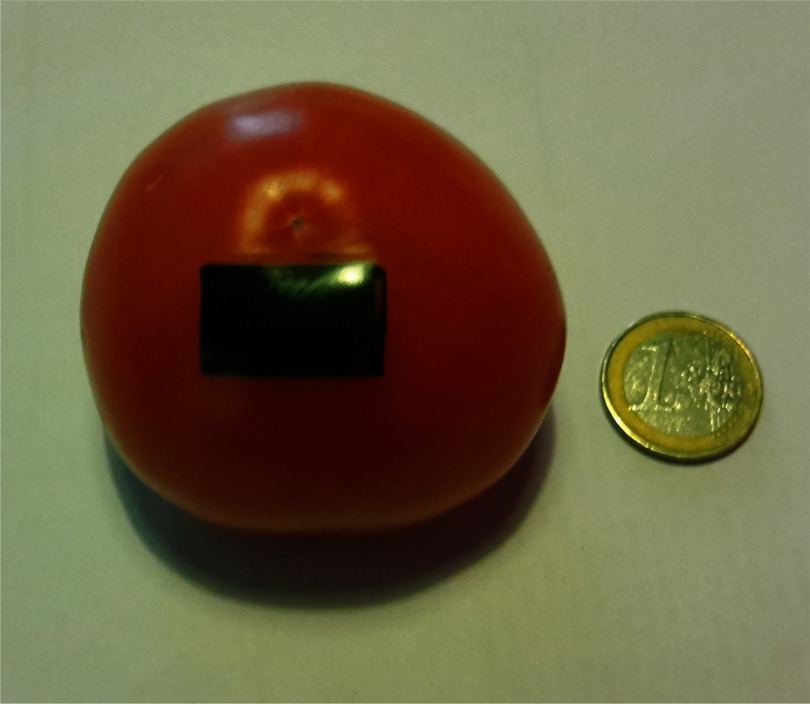
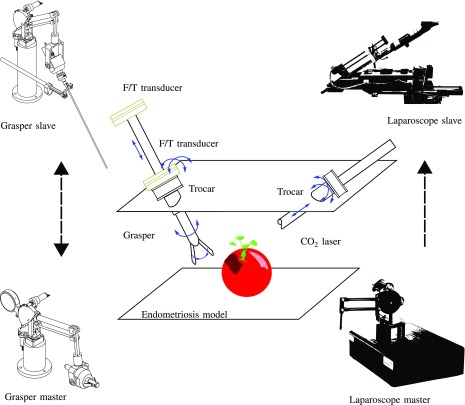
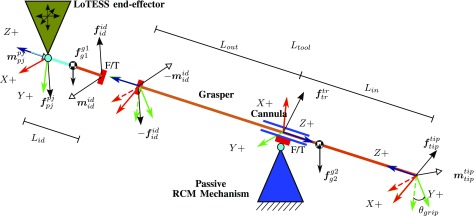
Methods: A new training exercise, "endometriosis surgery exercise" (ESE) has been devised approximating the setting for monocular robotic endometriosis treatment. A bimanual bilateral teleoperation setup was designed for laparoscopic laser surgery. Haptic guidance and haptic feedback are, respectively, offered to the operator. User experiments have been conducted to assess the validity of ESE and examine possible advantages of haptic technology during execution of bimanual surgery.
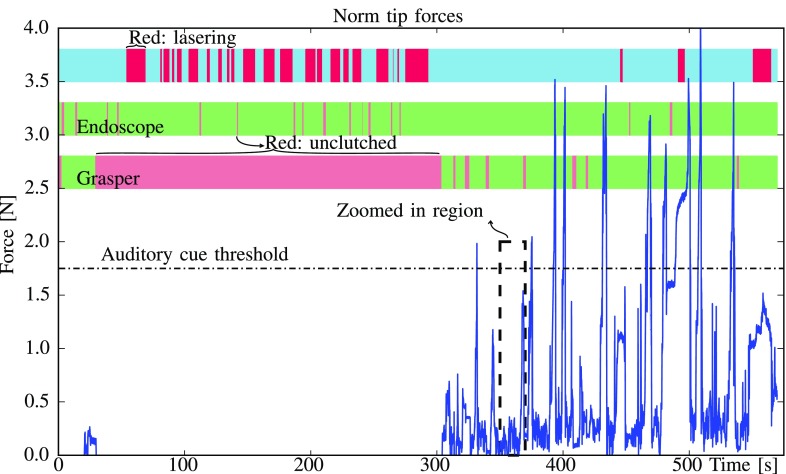
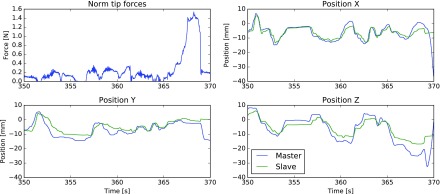
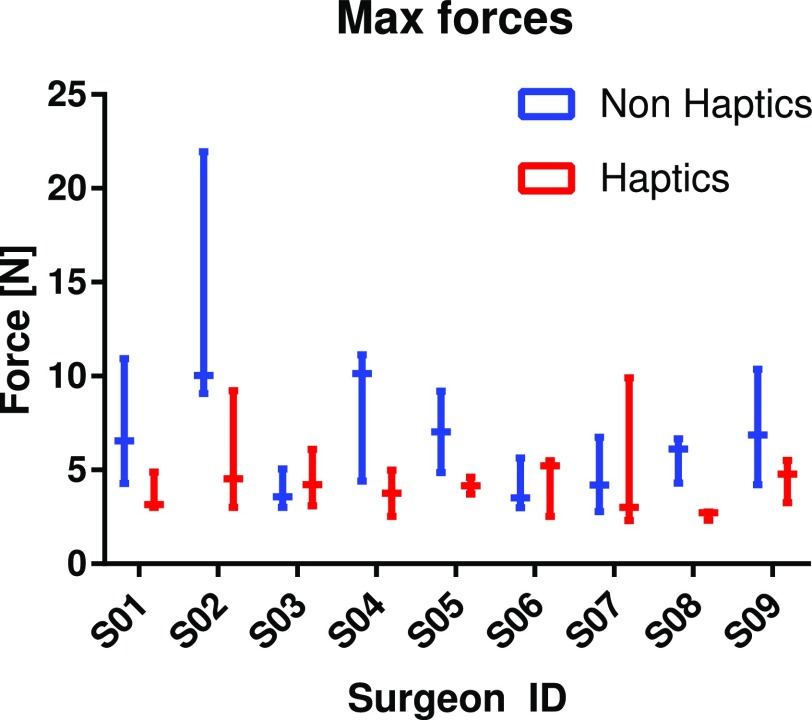
Results: Content and face validity of ESE were established by participating surgeons. Surgeons suggested ESE also as a mean to train lasering skills, and interaction forces on endometriotic tissue were found to be significantly lower when a bilateral controller is used. Collisions between instruments and the environment were less frequent and so were situations marked as potentially dangerous.
Conclusion: This study provides some promising results suggesting that haptics may offer a distinct advantage in complex robotic interventions were fragile tissue is manipulated.
Significance: Patients need to know whether it should be incorporated. Improved understanding of the value of haptics is important as current commercial surgical robots are widely used but do not offer haptics.
Figures

References
-
- Melvin W. S. and Kirakopolous A., The SAGES Manual: Volume 1 Basic Laparoscopy and Endoscopy. New York, NY, USA: Springer-Verlag, 2012, ch. Robotics in Laparoscopic and Thoracoscopic Surgery, pp. 191–203.
-
- Nezhat C. R. et al., “Robotic-assisted laparoscopy vs conventional laparoscopy for the treatment of advanced stage endometriosis,” J. Minimally Invasive Gynecology, vol. 22, no. 1, pp. 40–44, 2015. - PubMed
-
- Advincula A. and Song A., “The role of robotic surgery in gynecology,” Current Opinion Obstetrics Gynecology, vol. 19, no. 4, pp. 331–336, 2007. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
