

Effectiveness and limitations of an incident-reporting system analyzed by local clinical safety leaders in a tertiary hospital: Prospective evaluation through real-time observations of patient safety incidents
- PMID: 30235764
- PMCID: PMC6160204
- DOI: 10.1097/MD.0000000000012509
Effectiveness and limitations of an incident-reporting system analyzed by local clinical safety leaders in a tertiary hospital: Prospective evaluation through real-time observations of patient safety incidents
Abstract
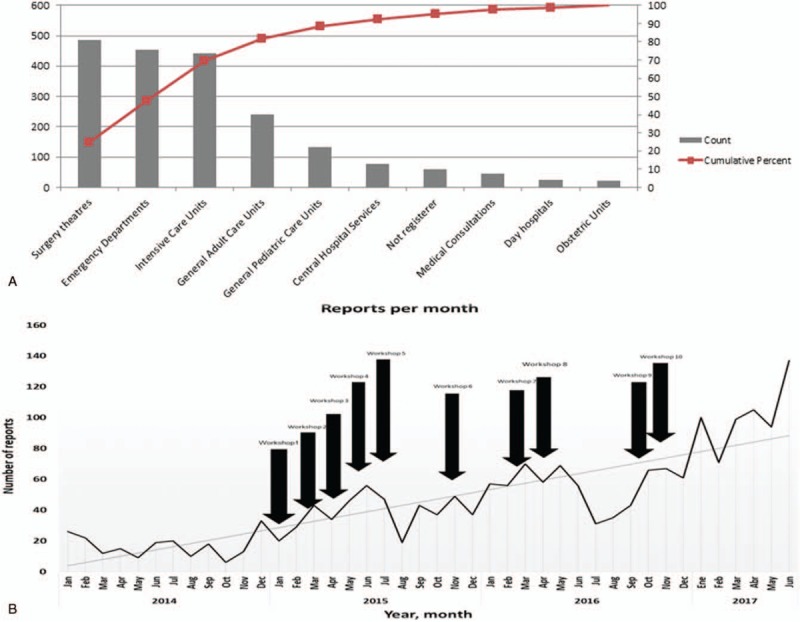
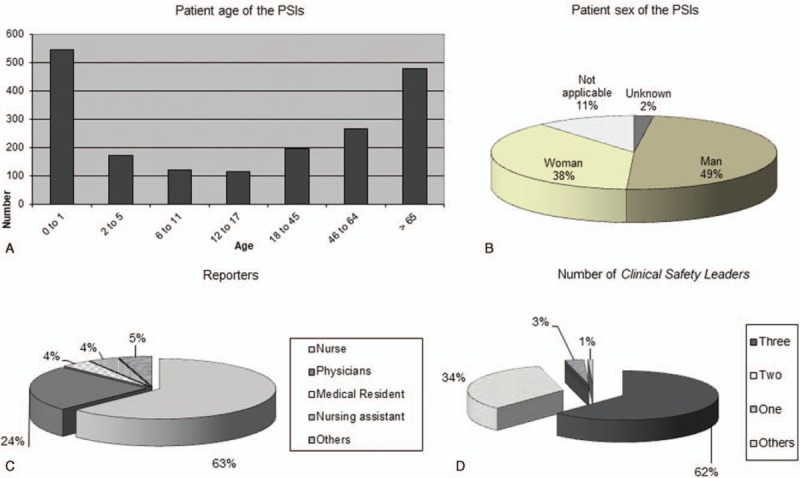
The effectiveness of a hospital incident-reporting system (IRS) on improve patient safety is unclear. This study objective was to assess which implemented improvement actions after the analysis of the incidents reported were effective in reduce near-misses or adverse events.Patient safety incidents (PSIs), near misses and adverse events, notified to the IRS were analyzed by local clinical safety leaders (CSLs) who propose and implement improvement actions. The local CSLs received training workshops in patient safety and analysis tools. Following the notification of a PSI in the IRS, prospective real-time observations with external staff were planned to record and rated the frequency of that PSI. This methodology was repeated after the implementation of the improvement actions.Ultimately, 1983 PSIs were identified. Surgery theaters, emergency departments, intensive care units, and general adult care units comprised 82% of all PSIs. The PSI rate increased from 0.39 to 3.4 per 1000 stays in 42 months. A significant correlation was found between the reporting rate per month and the number of workshop-trained local CSLs (Spearman coefficient = 0.874; P = .003). A total of 24,836 real-time observations showed a statistically significant reduction in PSIs observed in 63.15% (categories: medication P = .044; communication P = .037; technology P = .009) of the implemented improvements actions, but not in the organization category (P = .094). In the multivariate analyses, the following factors were associated with the reduction in near misses or adverse events after the implementation of the improvement actions: "adverse event" type of PSI (odds ratio [OR], 3.67; 95% confidence interval [CI], 1.93-5.74), "disussion group" type of analysis (OR, 2.45; 95% CI, 1.52-3.76), and root cause type of analysis (OR, 2.32; 95% CI: 1.17-3.90).The implementation of a hospital IRS, together with the systematization of the method and analysis of PSIs by workshop-trained local CSLs led to an important reduction in the frequency of PSIs.
Conflict of interest statement
The authors have no other conflicts of interest to disclose. The authors have no funding to disclose.
Figures
References
-
- Institute of Medicine. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press; 1999.
-
- Müller M. Risk and error management: can medicine benefit from lessons learned in aviation? [in German]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2015;58:95–9. - PubMed
-
- Brunsveld-Reinders AH, Arbous MS, De Vos R, et al. Incident and error reporting systems in intensive care: a systematic review of the literature. Int J Qual Health Care 2016;28:2–13. - PubMed
-
- Sistema de Notificación y Aprendizaje para la Seguridad del Paciente (SiNASP). Available at: https://www.sinasp.es/. Accessed September 9, 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
