

Perinatal death beyond 41 weeks pregnancy: an evaluation of causes and substandard care factors as identified in perinatal audit in the Netherlands
- PMID: 30236080
- PMCID: PMC6149052
- DOI: 10.1186/s12884-018-1973-0
Perinatal death beyond 41 weeks pregnancy: an evaluation of causes and substandard care factors as identified in perinatal audit in the Netherlands
Abstract
Background: Late- and postterm pregnancy are associated with adverse perinatal outcomes, like perinatal death. We evaluated causes of death and substandard care factors (SSFs) in term and postterm perinatal death.
Methods: We used data from the Perinatal Audit Registry of the Netherlands (PARS). Women with a term perinatal death registered in PARS were stratified by gestational age into early-/full-term (37.0-40.6) and late-/postterm (≥41.0 weeks) death. Cause of death and SSFs ≥41 weeks were scored and classified by the local perinatal audit teams.
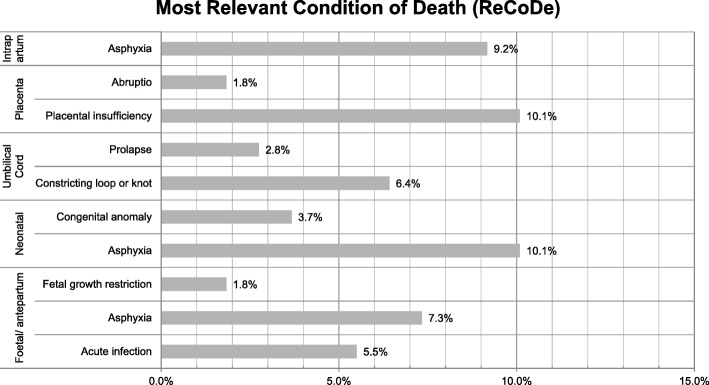
Results: During 2010-2012, 947/479,097 (0.21%) term deaths occurred, from which 707 cases (75%) were registered and could be used for analyses. Five hundred ninety-eight early-/full-term and 109 late-/postterm audited deaths were registered in the PARS database. Of all audited cases of perinatal death in the PARS database, 55.2% in the early-/fullterm group occurred antepartum compared to 42.2% in the late-/postterm group, while intrapartum death occurred in 7.2% in the early-/full-term group compared to 19.3% in the late-/postterm group in the audited cases from the PARS database. According to the local perinatal audit, the most relevant causes of perinatal death ≥41 weeks were antepartum asphyxia (7.3%), intrapartum asphyxia (9.2%), neonatal asphyxia (10.1%) and placental insufficiency (10.1%). In the group with perinatal death ≥41 weeks there was ≥1SSF identified in 68.8%. The most frequent SSFs concerned inadequate cardiotocography (CTG) evaluation and/or classification (10.1%), incomplete registration or documentation in medical files (4.6%) or inadequate action on decreased foetal movements (4.6%).
Conclusions: In the Netherlands Perinatal Audit Registry, stillbirth occurred relatively less often antepartum and more often intrapartum in pregnancies ≥41 weeks compared to pregnancies at 37.0-40.6 weeks in the audited cases from the PARS database. Foetal, intrapartum and neonatal asphyxia were identified more frequently as cause of death in pregnancies ≥41 weeks. The most identified SSFs related to death in pregnancies ≥41 weeks concerned inadequate CTG monitoring (evaluation, classification, registration or documentation) and inadequate action on decreased foetal movements.
Keywords: CTG; Delivery; Foetal monitoring; Late-term pregnancy; Mortality; Postterm pregnancy; Pregnancy; Stillbirth.
Conflict of interest statement
Ethics approval and consent to participate
No ethical approval was needed according to the Dutch Central Committee of Human Research, because of the retrospective cohort study.
Consent for publication
Not applicable.
Competing interests
JvD is a member of the editorial board (associate editor) of the BMC Pregnancy and Childbirth. All other authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Vayssiere C, Haumonte JB, Chantry A, Coatleven F, Debord MP, Gomez C, Le Ray C, Lopez E, Salomon LJ, Senat MV, et al. Prolonged and post-term pregnancies: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF) Eur J Obstet Gynecol Reprod Biol. 2013;169(1):10–16. doi: 10.1016/j.ejogrb.2013.01.026. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
