

Frailty trajectories to identify end of life: a longitudinal population-based study
- PMID: 30236103
- PMCID: PMC6148780
- DOI: 10.1186/s12916-018-1148-x
Frailty trajectories to identify end of life: a longitudinal population-based study
Abstract
Background: Timely recognition of the end of life allows patients to discuss preferences and make advance plans, and clinicians to introduce appropriate care. We examined changes in frailty over 1 year, with the aim of identifying trajectories that could indicate where an individual is at increased risk of all-cause mortality and may require palliative care.
Methods: Electronic health records from 13,149 adults (cases) age 75 and over who died during a 1-year period (1 January 2015 to 1 January 2016) were age, sex and general practice matched to 13,149 individuals with no record of death over the same period (controls). Monthly frailty scores were obtained for 1 year prior to death for cases, and from 1 January 2015 to 1 January 2016 for controls using the electronic frailty index (eFI; a cumulative deficit measure of frailty, available in most English primary care electronic health records, and ranging in value from 0 to 1). Latent growth mixture models were used to investigate longitudinal patterns of change and associated impact on mortality. Cases were reweighted to the population level for tests of diagnostic accuracy.
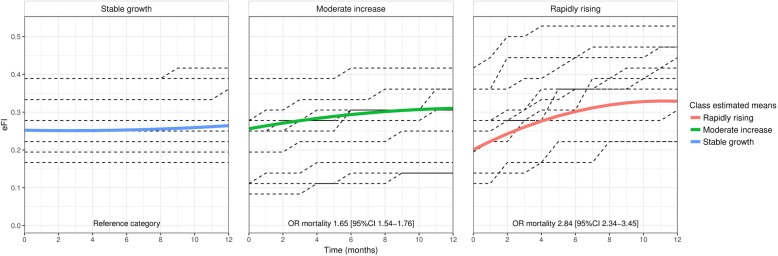
Results: Three distinct frailty trajectories were identified. Rapidly rising frailty (initial increase of 0.022 eFI per month before slowing from a baseline eFI of 0.21) was associated with a 180% increase in mortality (OR 2.84, 95% CI 2.34-3.45) for 2.2% of the sample. Moderately increasing frailty (eFI increase of 0.007 per month, with baseline of 0.26) was associated with a 65% increase in mortality (OR 1.65, 95% CI 1.54-1.76) for 21.2% of the sample. The largest (76.6%) class was stable frailty (eFI increase of 0.001 from a baseline of 0.26). When cases were reweighted to population level, rapidly rising frailty had 99.1% specificity and 3.2% sensitivity (positive predictive value 19.8%, negative predictive value 93.3%) for predicting individual risk of mortality.
Conclusions: People aged over 75 with frailty who are at highest risk of death have a distinctive frailty trajectory in the last 12 months of life, with a rapid initial rise from a low baseline, followed by a plateau. Routine measurement of frailty can be useful to support clinicians to identify people with frailty who are potential candidates for palliative care, and allow time for intervention.
Keywords: End of life; Frailty; Geriatrics; Palliative care; Primary care.
Conflict of interest statement
Ethics approval and consent to participate
Approval for this study was granted by the ResearchOne ethical review panel with oversight from the UK NHS Health Research Authority and the UK Government Health and Social Care Information Centre Confidentiality Advisory Group. ResearchOne was approved by the UK National Health Service (NHS) National Research Ethics Service (11/NE/0184).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Evaluating frailty scores to predict mortality in older adults using data from population based electronic health records: case control study.Age Ageing. 2018 Jul 1;47(4):564-569. doi: 10.1093/ageing/afy022. Age Ageing. 2018. PMID: 29546362 Free PMC article.
-
Longitudinal trajectories of frailty are associated with short-term mortality in older people: a joint latent class models analysis using 2 UK primary care databases.J Clin Epidemiol. 2024 Sep;173:111442. doi: 10.1016/j.jclinepi.2024.111442. Epub 2024 Jun 26. J Clin Epidemiol. 2024. PMID: 38942178
-
Development and validation of an electronic frailty index using routine primary care electronic health record data.Age Ageing. 2016 May;45(3):353-60. doi: 10.1093/ageing/afw039. Epub 2016 Mar 3. Age Ageing. 2016. PMID: 26944937 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Development, Validation, and Application of the Electronic Frailty Index: A Scoping Review.J Am Med Dir Assoc. 2025 Jun;26(6):105577. doi: 10.1016/j.jamda.2025.105577. Epub 2025 May 14. J Am Med Dir Assoc. 2025. PMID: 40164233
Cited by
-
Timing of GP end-of-life recognition in people aged ≥75 years: retrospective cohort study using data from primary healthcare records in England.Br J Gen Pract. 2020 Nov 26;70(701):e874-e879. doi: 10.3399/bjgp20X713417. Print 2020 Dec. Br J Gen Pract. 2020. PMID: 33139331 Free PMC article.
-
The relationship between deprivation and frailty trajectories over 1 year and at the end of life: a case-control study.J Public Health (Oxf). 2022 Dec 1;44(4):844-850. doi: 10.1093/pubmed/fdab320. J Public Health (Oxf). 2022. PMID: 34542629 Free PMC article.
-
Frailty trajectories and associated factors in the years prior to death: evidence from 14 countries in the Survey of Health, Aging and Retirement in Europe.BMC Geriatr. 2023 Jan 27;23(1):49. doi: 10.1186/s12877-023-03736-1. BMC Geriatr. 2023. PMID: 36703138 Free PMC article.
-
Prognostic Factors of Physical Function Decline Among Middle-Aged Adults With HIV.Open Forum Infect Dis. 2025 May 27;12(6):ofaf311. doi: 10.1093/ofid/ofaf311. eCollection 2025 Jun. Open Forum Infect Dis. 2025. PMID: 40519631 Free PMC article.
-
Frailty trajectories in three longitudinal studies of aging: Is the level or the rate of change more predictive of mortality?Age Ageing. 2021 Nov 10;50(6):2174-2182. doi: 10.1093/ageing/afab106. Age Ageing. 2021. PMID: 34120182 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
