

Positive Pressure Ventilation in the Cardiac Intensive Care Unit
- PMID: 30236315
- PMCID: PMC11032173
- DOI: 10.1016/j.jacc.2018.06.074
Positive Pressure Ventilation in the Cardiac Intensive Care Unit
Abstract
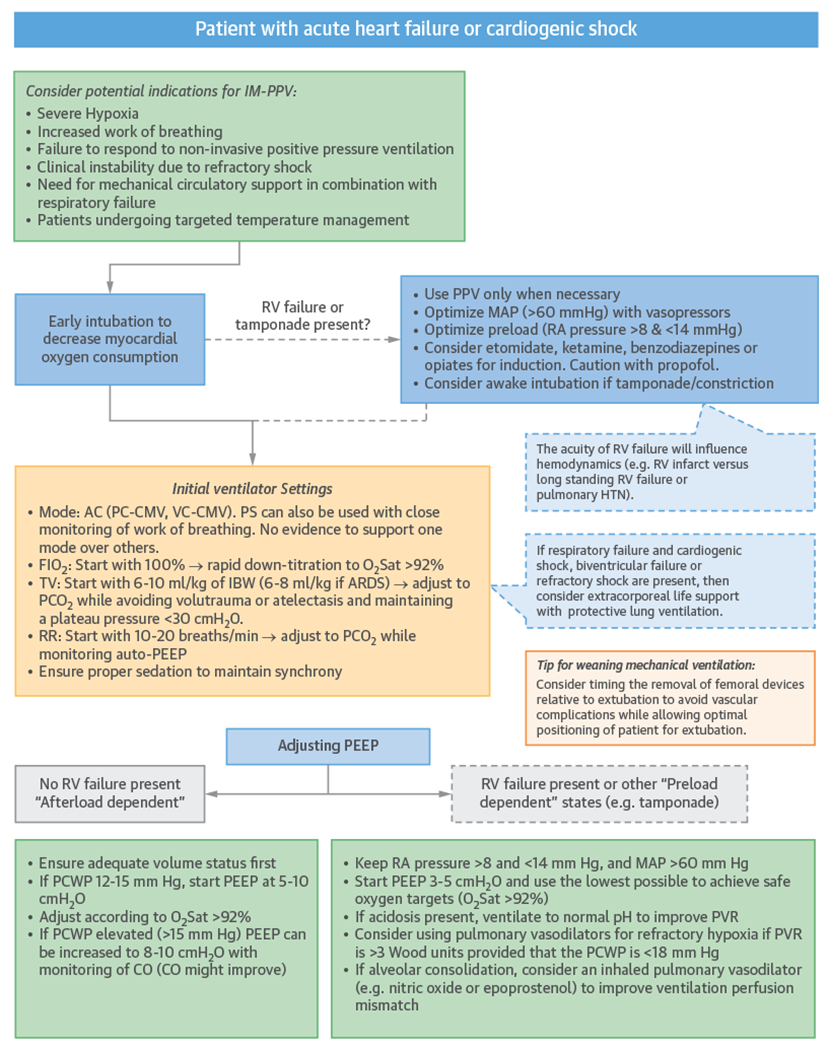
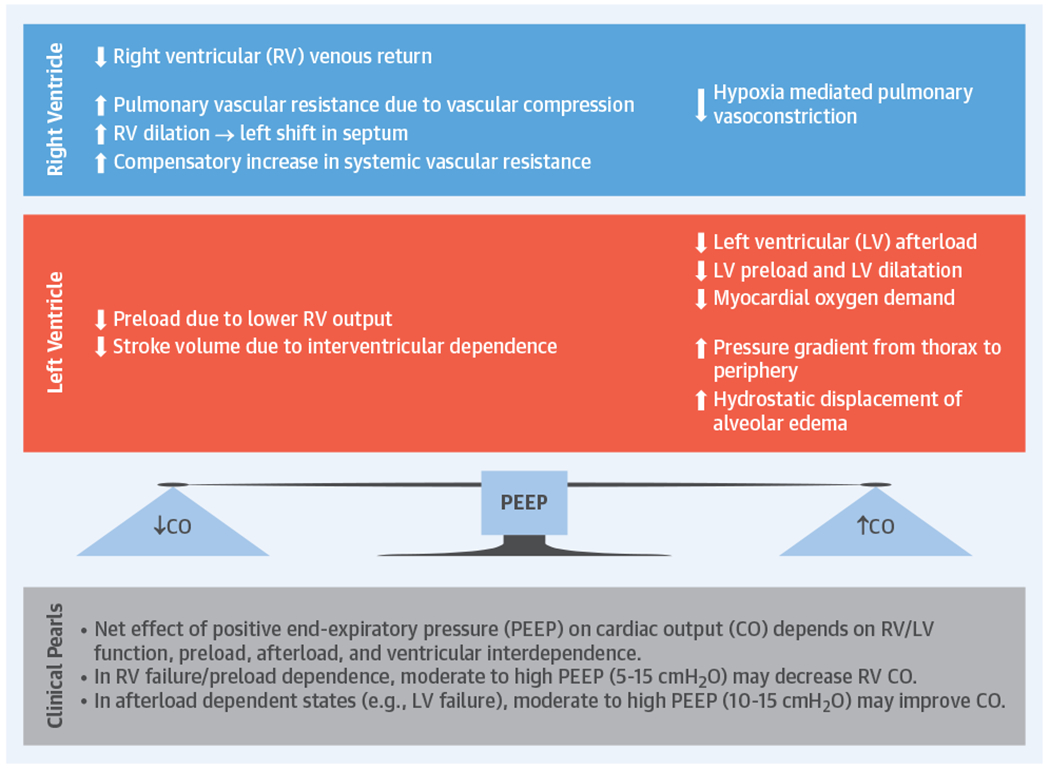
Contemporary cardiac intensive care units (CICUs) provide care for an aging and increasingly complex patient population. The medical complexity of this population is partly driven by an increased proportion of patients with respiratory failure needing noninvasive or invasive positive pressure ventilation (PPV). PPV often plays an important role in the management of patients with cardiogenic pulmonary edema, cardiogenic shock, or cardiac arrest, and those undergoing mechanical circulatory support. Noninvasive PPV, when appropriately applied to selected patients, may reduce the need for invasive mechanical PPV and improve survival. Invasive PPV can be lifesaving, but has both favorable and unfavorable interactions with left and right ventricular physiology and carries a risk of complications that influence CICU mortality. Effective implementation of PPV requires an understanding of the underlying cardiac and pulmonary pathophysiology. Cardiologists who practice in the CICU should be proficient with the indications, appropriate selection, potential cardiopulmonary interactions, and complications of PPV.
Keywords: coronary intensive care unit; heart failure; mechanical ventilation; noninvasive ventilation; pulmonary edema; respiratory failure.
Copyright © 2018 American College of Cardiology Foundation. All rights reserved.
Figures
References
-
- Morrow DA, Fang JC, Fintel DJ, et al. Evolution of critical care cardiology: transformation of the cardiovascular intensive care unit and the emerging need for new medical staffing and training models: a scientific statement from the American Heart Association. Circulation 2012;126:1408–28. - PubMed
-
- Katz JN, Shah BR, Volz EM, et al. Evolution of the coronary care unit: clinical characteristics and temporal trends in healthcare delivery and outcomes. Crit Care Med 2010;38:375–81. - PubMed
-
- Morrow DA. Trends in cardiac critical care: reshaping the cardiac intensive care unit. Circ Cardiovasc Qual Outcomes 2017;10:e004010. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
