

Home-based versus office-based biofeedback therapy for constipation with dyssynergic defecation: a randomised controlled trial
- PMID: 30236904
- PMCID: PMC6206847
- DOI: 10.1016/S2468-1253(18)30266-8
Home-based versus office-based biofeedback therapy for constipation with dyssynergic defecation: a randomised controlled trial
Abstract
Background: Office-based biofeedback therapy is effective for constipation with dyssynergic defecation, but must be performed by skilled staff, is only available in selected centres, and requires multiple visits. The efficacy of home-based biofeedback therapy is unknown. We compared clinical and subjective outcomes with home-based and office-based approaches.
Methods: In this randomised controlled trial, eligible patients were adult outpatients (age 18-80 years) who met the Rome III criteria for functional constipation and who had been referred to a tertiary-care centre after non-response to routine management, and who had dyssynergic defecation. Patients were randomly assigned according to a schedule generated in advance by the study biostatistician, in permuted blocks of four, to receive office-based or home-based biofeedback therapy. Office-based biofeedback comprised therapist-guided pelvic floor training for six sessions over 3 months (visits every 2 weeks). Home-based biofeedback comprised 20 min self-training sessions twice per day, in which a self-inserted probe was used to provide visual feedback via a handheld monitoring device of anal sphincter pressure and push effort. Patients recorded in diaries the time of each defecation attempt, stool consistency, straining effort, feeling of incomplete evacuation, need for digital assistance with stooling, and satisfaction with bowel function, from 1 week before enrolment to the end of follow-up. Treatment responders were defined post hoc as those with normalisation of dyssynergic defecation and an increase in the number of complete spontaneous bowel movements per week by 3 months. Cost outcomes calculated from health-care costs and loss of salary were assessed from hospital billing and medical records and questionnaires. Primary outcome measures were the presence of a dyssynergic pattern during attempted defecation, balloon expulsion time, the number of complete spontaneous bowel movements per week, and satisfaction with bowel function, assessed by intention to treat (non-inferiority) and per protocol. This trial is registered with ClinicalTrials.gov, number NCT03202771.
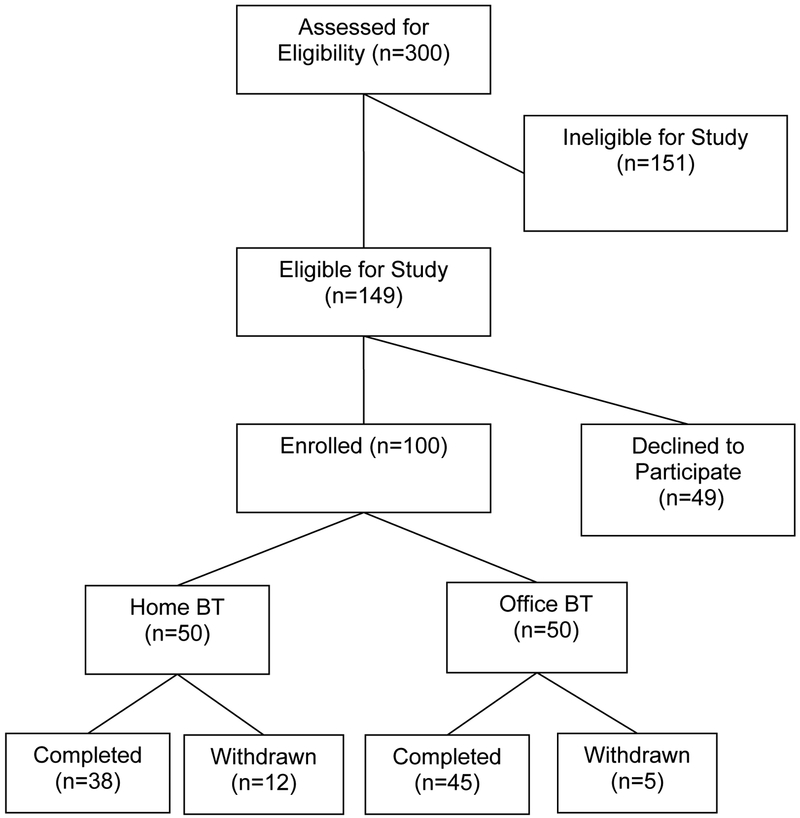
Findings: Of 300 patients screened we enrolled 100, from Jan 7, 2005, to Jan 31, 2010. 83 patients completed training (38 [76%] of 50 in the home-based biofeedback group and 45 [90%] of 50 in the office-based biofeedback group). 34 (68%) patients in the home-based group and 35 (70%) in the office-based group were classified as responders. All primary outcomes improved significantly from baseline in the two treatment groups (all p<0·0001). Home-based biofeedback therapy was non-inferior to office-based therapy for number of complete spontaneous bowel movements per week, satisfaction with bowel function, and balloon expulsion time in the intention-to-treat and per-protocol analyses, and for dyssynergia in the per-protocol analysis. No adverse events were reported. The median cost of home-based biofeedback therapy was significantly lower than that for office-based treatment (US$1081·70, IQR 794·90-1399·30 vs $1942·50, 1621·70-2369·00, p=0·009).
Interpretation: Home-based and office-based biofeedback therapy for dyssynergic defecation improved bowel symptoms and physiology with similar efficacy. A home-based programme could substantially broaden the availability and use of this treatment.
Funding: National Institutes of Health.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Comment in
-
Home-based biofeedback for dyssynergic defecation.Lancet Gastroenterol Hepatol. 2018 Nov;3(11):733-734. doi: 10.1016/S2468-1253(18)30284-X. Epub 2018 Sep 18. Lancet Gastroenterol Hepatol. 2018. PMID: 30236903 No abstract available.
References
-
- Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol 2004;99:750–9. - PubMed
-
- Rao SSC, Camilleri M. Clinical approach to constipation In Yamada’s Text Book of Gastroenterology, 6th Edition, Edited by Podolsky D et al., Chapter 42, John Wiley & Sons, Ltd; 2016. Pp 757–780.
-
- Mertz H, Naliboff B, Mayer E. Physiology of refractory chronic constipation. Am J Gastroenterol 1999;94:609–15. - PubMed
-
- Bharucha AE, Dorn SD, Lembo A, Pressman A. American Gastroenterological Association medical position statement on constipation. Gastroenterology 2013;144:211–17. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
