

"Fat Shadows" From DXA for the Qualitative Assessment of Lipodystrophy: When a Picture Is Worth a Thousand Numbers
- PMID: 30237235
- PMCID: PMC6150431
- DOI: 10.2337/dc18-0978
"Fat Shadows" From DXA for the Qualitative Assessment of Lipodystrophy: When a Picture Is Worth a Thousand Numbers
Abstract
Objective: Lipodystrophy syndromes are a heterogeneous group of disorders associated with selective absence of fat. Currently, the diagnosis is established only clinically.
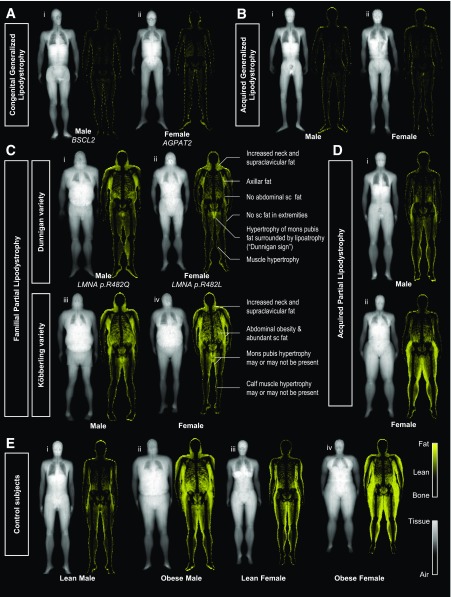
Research design and methods: We developed a new method from DXA scans called a "fat shadow," which is a color-coded representation highlighting only the fat tissue. We conducted a blinded retrospective validation study to assess its usefulness for the diagnosis of lipodystrophy syndromes.
Results: We evaluated the fat shadows from 16 patients (11 female and 5 male) with generalized lipodystrophy (GL), 57 (50 female and 7 male) with familial partial lipodystrophy (FPLD), 2 (1 female and 1 male) with acquired partial lipodystrophy, and 126 (90 female and 36 male) control subjects. FPLD was differentiated from control subjects with 85% sensitivity and 96% specificity (95% CIs 72-93 and 91-99, respectively). GL was differentiated from nonobese control subjects with 100% sensitivity and specificity (95% CIs 79-100 and 92-100, respectively).
Conclusions: Fat shadows provided sufficient qualitative information to infer clinical phenotype and differentiate these patients from appropriate control subjects. We propose that this method could be used to support the diagnosis.
© 2018 by the American Diabetes Association.
Figures
References
-
- Huang-Doran I, Sleigh A, Rochford JJ, O’Rahilly S, Savage DB. Lipodystrophy: metabolic insights from a rare disorder. J Endocrinol 2010;207:245–255 - PubMed
-
- Guillín-Amarelle C, Sánchez-Iglesias S, Castro-Pais A, et al. . Type 1 familial partial lipodystrophy: understanding the Köbberling syndrome. Endocrine 2016;54:411–421 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
