

Daratumumab plus lenalidomide and dexamethasone versus lenalidomide and dexamethasone in relapsed or refractory multiple myeloma: updated analysis of POLLUX
- PMID: 30237262
- PMCID: PMC6269302
- DOI: 10.3324/haematol.2018.194282
Daratumumab plus lenalidomide and dexamethasone versus lenalidomide and dexamethasone in relapsed or refractory multiple myeloma: updated analysis of POLLUX
Abstract
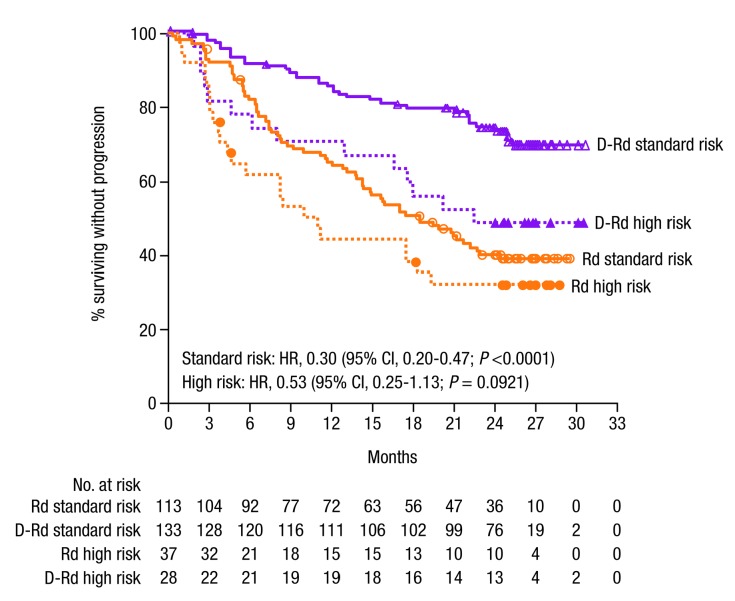
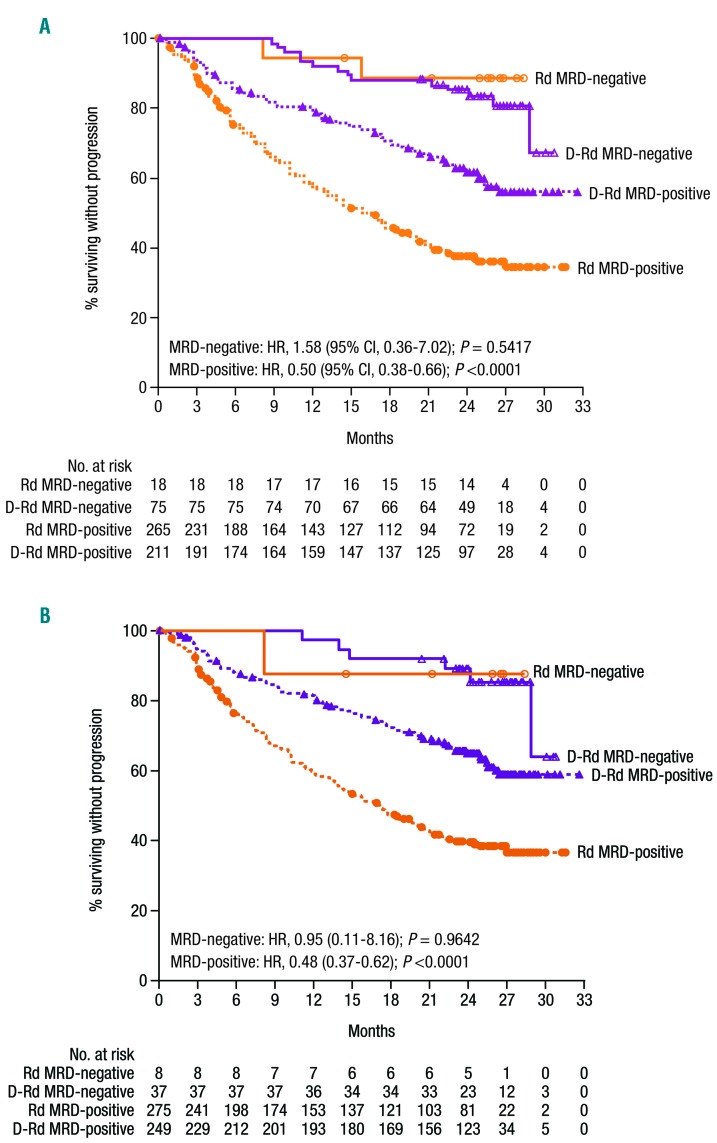
In the POLLUX study, daratumumab plus lenalidomide/dexamethasone significantly reduced risk of progression/death versus lenalidomide/dexamethasone alone in relapsed/refractory multiple myeloma. We provide one additional year of follow up and include the effect on minimal residual disease and in clinically relevant subgroups. After 25.4 months of follow up, daratumumab plus lenalidomide/dexamethasone prolonged progression-free survival versus lenalidomide/dexamethasone alone (median not reached vs 17.5 months; hazard ratio, 0.41; 95% confidence interval, 0.31-0.53; P<0.0001). The overall response rate was 92.9% versus 76.4%, and 51.2% versus 21.0% achieved a complete response or better, respectively (both P<0.0001). At the 10-5 sensitivity threshold, 26.2% versus 6.4% were minimal residual disease-negative, respectively (P<0.0001). Post hoc analyses of clinically relevant patient subgroups demonstrated that progression-free survival was significantly prolonged for daratumumab plus lenalidomide/dexamethasone versus lenalidomide/dexamethasone regardless of number of prior lines of therapy. Patients previously treated with lenalidomide or thalidomide and those refractory to bortezomib received similar benefits (all P<0.01). Treatment benefit with daratumumab plus lenalidomide/dexamethasone was maintained in high-risk patients (median progression-free survival 22.6 vs 10.2 months; hazard ratio, 0.53; 95% confidence interval, 0.25-1.13; P=0.0921) and patients with treatment-free intervals of >12 and ≤12 months and >6 and ≤6 months. No new safety signals were observed. In relapsed/refractory multiple myeloma patients, daratumumab plus lenalidomide/dexamethasone continued to improve progression-free survival and deepen responses versus lenalidomide/dexamethasone. Trial Registration: clinicaltrials.gov identifier: 02076009.
Copyright© 2018 Ferrata Storti Foundation.
Figures

References
-
- Moreau P, San Miguel J, Sonneveld P, et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl 4):iv52–iv61. - PubMed
-
- NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): multiple myeloma. Version 4. 2018. https://www.nccn.org/professionals/physician_gls/pdf/myeloma.pdf
-
- Lin P, Owens R, Tricot G, Wilson CS. Flow cytometric immunophenotypic analysis of 306 cases of multiple myeloma. Am J Clin Pathol. 2004;121(4):482–488. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
