

Safety of biweekly α1-antitrypsin treatment in the RAPID programme
- PMID: 30237305
- PMCID: PMC6557539
- DOI: 10.1183/13993003.00897-2018
Safety of biweekly α1-antitrypsin treatment in the RAPID programme
Abstract
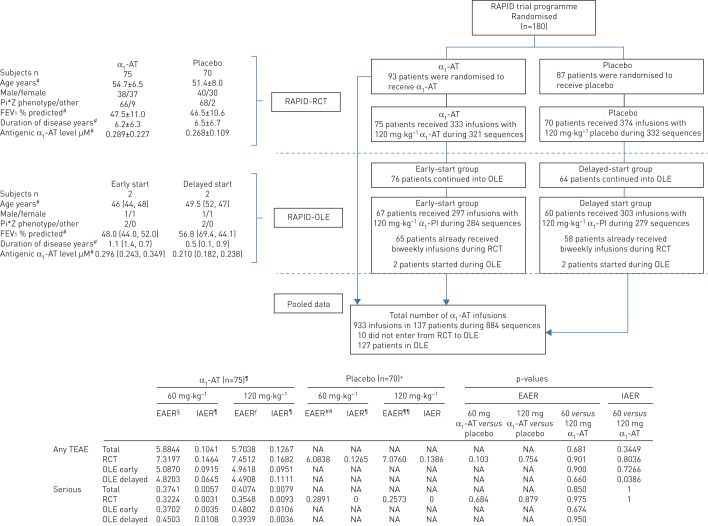
Administration of 120 mg·kg−1 α1-antitrypsin on a biweekly basis was safe and well tolerated
Trial registration: ClinicalTrials.gov NCT00261833 NCT00670007.
Conflict of interest statement
Conflict of interest: T. Greulich reports personal fees from AstraZeneca and GSK (lecture fees), Boehringer-Ingelheim, Chiesi, CSL Behring and Novartis (lecture fees, advisory board and travel support), and Mundipharma (lecture fees and advisory board); and grants and personal fees from Grifols (AATD-Labor, lecture fees and travel support), all outside the submitted work. Conflict of interest: J. Chlumsky reports honoraria for lectures organised by CSL Behring, and for lectures organised by Boehringer Ingelheim, outside the submitted work. Conflict of interest: M. Wencker reports support from conresp as a consultant to CSL Behring, during the conduct of the study. Conflict of interest: O. Vit reports support from CSL Behring, as employer and sponsor of the study. Conflict of interest: M. Fries reports support from CSL Behring, as employer and sponsor of the study. Conflict of interest: T. Chung reports support from CSL Behring, as employer and sponsor of the study. Conflict of interest: A. Shebl reports support from CSL Behring, as employer and sponsor of the study. Conflict of interest: C. Vogelmeier reports grants and personal fees from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Grifols and Novartis; personal fees from CSL Behring, Chiesi, Menarini, Mundipharma, Teva and Cipla; and grants from Bayer-Schering, MSD and Pfizer, all outside the submitted work. Conflict of interest: K.R. Chapman reports grants and personal fees from AstraZeneca, Boehringer Ingelheim, CSL Behring, Grifols, Sanofi, Genentech, Kamada, Roche and Novartis; grants from Baxter, GlaxoSmithKline, Amgen, Shire and Octapharma; personal fees from Merck; and the CIHR-GSK Research Chair in Respiratory Health Care Delivery, UHN, all during the conduct of the study. Conflict of interest: N.G. McElvaney reports research grants for carrying out the original RAPID and RAPID OLE studies from CSL Behring, during the conduct of the study; and personal fees from CSL Behring (advisory board), outside the submitted work.
Figures
References
-
- Greene CM, Marciniak SJ, Teckman J, et al. . α1-Antitrypsin deficiency. Nat Rev Dis Primers 2016; 2: 16051. - PubMed
-
- Piras B, Ferrarotti I, Lara B, et al. . Clinical phenotypes of Italian and Spanish patients with α1-antitrypsin deficiency. Eur Respir J 2013; 42: 54–64. - PubMed
-
- Chapman KR, Burdon JG, Piitulainen E, et al. . Intravenous augmentation treatment and lung density in severe α1 antitrypsin deficiency (RAPID): a randomised, double-blind, placebo-controlled trial. Lancet 2015; 386: 360–368. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical