

Reproducibility study on myocardial strain assessment using fast-SENC cardiac magnetic resonance imaging
- PMID: 30237411
- PMCID: PMC6147889
- DOI: 10.1038/s41598-018-32226-3
Reproducibility study on myocardial strain assessment using fast-SENC cardiac magnetic resonance imaging
Abstract
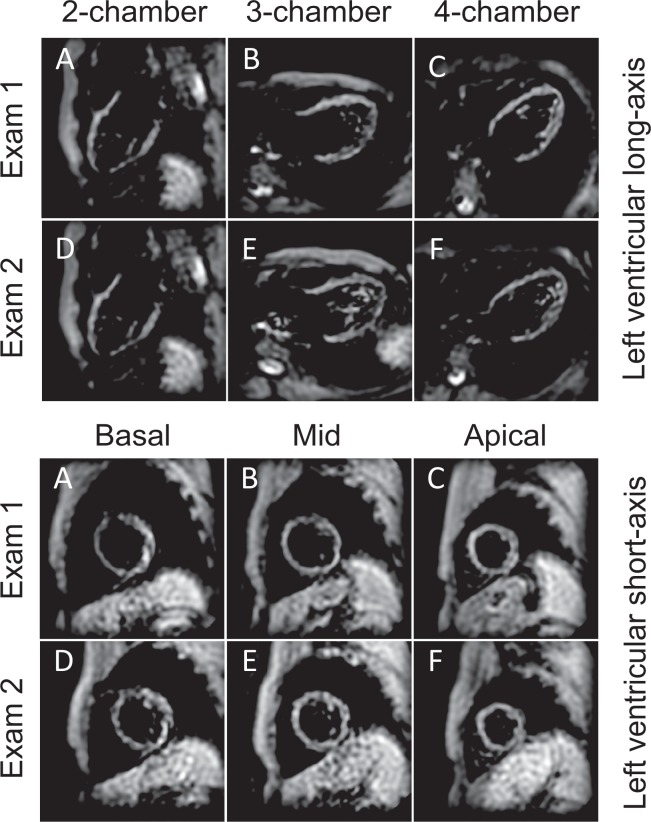
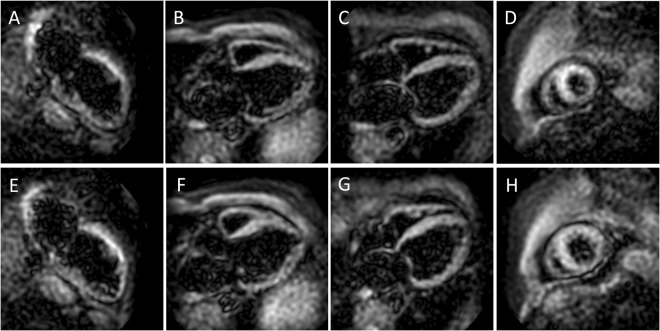
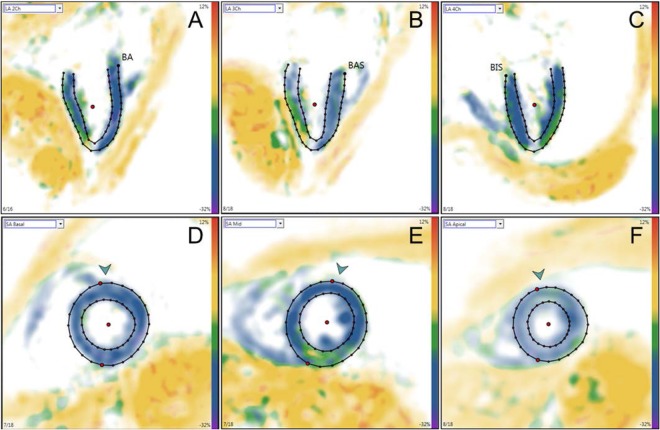
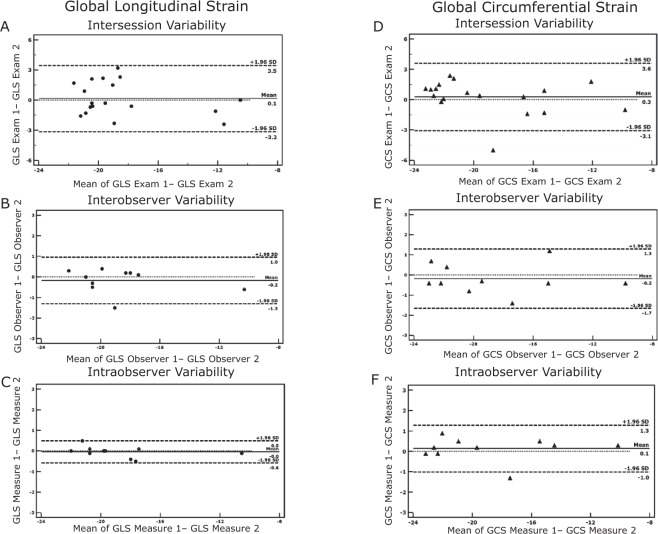
Myocardial strain is a well validated parameter for estimating left ventricular (LV) performance. The aim of our study was to evaluate the inter-study as well as intra- and interobserver reproducibility of fast-SENC derived myocardial strain. Eighteen subjects (11 healthy individuals and 7 patients with heart failure) underwent a cardiac MRI examination including fast-SENC acquisition for evaluating left ventricular global longitudinal (GLS) and circumferential strain (GCS) as well as left ventricular ejection fraction (LVEF). The examination was repeated after 63 [range 49‒87] days and analyzed by two experienced observers. Ten datasets were repeatedly assessed after 1 month by the same observer to test intraobserver variability. The reproducibility was measured using the intraclass correlation coefficient (ICC) and Bland-Altman analysis. Patients with heart failure demonstrated reduced GLS and GCS compared to healthy controls (-15.7 ± 3.7 vs. -20.1 ± 1.4; p = 0.002 for GLS and -15.3 ± 3.7 vs. -21.4 ± 1.1; p = 0.001 for GCS). The test-retest analysis showed excellent ICC for LVEF (0.92), GLS (0.94) and GCS (0.95). GLS exhibited excellent ICC (0.99) in both intra- and interobserver variability analysis with very narrow limits of agreement (-0.6 to 0.5 for intraobserver and -1.3 to 0.96 for interobserver agreement). Similarly, GCS showed excellent ICC (0.99) in both variability analyses with narrow limits of agreement (-1.1 to 1.2 for intraobserver and -1.7 to 1.3 for interobserver agreement), whereas LVEF showed larger limits of agreement (-14.4 to 10.1). The analysis of fast-SENC derived myocardial strain using cardiac MRI provides a highly reproducible method for assessing LV functional performance.
Conflict of interest statement
S.K., A.P. and K.K. received an unrestricted research grant by Philips Healthcare and a research grant from Myocardial Solutions. B.S. and C.S. are employees of Philips Healthcare. T.L., S.K., A.S., E.P.K. and B.P. received support from the DZHK (German Centre for Cardiovascular Research). S.K. owns stock options of Myocardial Solutions. The remaining authors declare that they have no competing interests.
Figures

Similar articles
-
Comparison of feature tracking, fast-SENC, and myocardial tagging for global and segmental left ventricular strain.ESC Heart Fail. 2020 Apr;7(2):523-532. doi: 10.1002/ehf2.12576. Epub 2019 Dec 4. ESC Heart Fail. 2020. PMID: 31800152 Free PMC article.
-
Effect of comprehensive initial training on the variability of left ventricular measures using fast-SENC cardiac magnetic resonance imaging.Sci Rep. 2019 Aug 21;9(1):12223. doi: 10.1038/s41598-019-48685-1. Sci Rep. 2019. PMID: 31434950 Free PMC article. Clinical Trial.
-
Echocardiography and cardiovascular magnetic resonance based evaluation of myocardial strain and relationship with late gadolinium enhancement.J Cardiovasc Magn Reson. 2019 Aug 8;21(1):46. doi: 10.1186/s12968-019-0559-y. J Cardiovasc Magn Reson. 2019. PMID: 31391036 Free PMC article.
-
MRI-Derived Myocardial Strain Measures in Normal Subjects.JACC Cardiovasc Imaging. 2018 Feb;11(2 Pt 1):196-205. doi: 10.1016/j.jcmg.2016.12.025. Epub 2017 May 17. JACC Cardiovasc Imaging. 2018. PMID: 28528164
-
Imaging and heart failure: myocardial strain.Curr Opin Cardiol. 2019 Sep;34(5):490-494. doi: 10.1097/HCO.0000000000000653. Curr Opin Cardiol. 2019. PMID: 31219880 Review.
Cited by
-
Variability of Myocardial Strain During Isometric Exercise in Subjects With and Without Heart Failure.Front Cardiovasc Med. 2020 Jun 30;7:111. doi: 10.3389/fcvm.2020.00111. eCollection 2020. Front Cardiovasc Med. 2020. PMID: 32714945 Free PMC article.
-
A multicenter study on the comparability of myocardial strain values acquired with different CMR scanners and analyzed with different post-processing software: insights into the "Traveling Volunteers" study.Int J Comput Assist Radiol Surg. 2025 Aug 30. doi: 10.1007/s11548-025-03499-7. Online ahead of print. Int J Comput Assist Radiol Surg. 2025. PMID: 40884734
-
Left and right ventricular strain using fast strain-encoded cardiovascular magnetic resonance for the diagnostic classification of patients with chronic non-ischemic heart failure due to dilated, hypertrophic cardiomyopathy or cardiac amyloidosis.J Cardiovasc Magn Reson. 2021 Apr 5;23(1):45. doi: 10.1186/s12968-021-00711-w. J Cardiovasc Magn Reson. 2021. PMID: 33823860 Free PMC article.
-
The Role of Cardiac Magnetic Resonance Imaging to Detect Cardiac Toxicity From Cancer Therapeutics.Curr Treat Options Cardiovasc Med. 2019 May 18;21(6):28. doi: 10.1007/s11936-019-0732-5. Curr Treat Options Cardiovasc Med. 2019. PMID: 31104180 Review.
-
Comparison of manual and artificial intelligence based quantification of myocardial strain by feature tracking-a cardiovascular MR study in health and disease.Eur Radiol. 2024 Feb;34(2):1003-1015. doi: 10.1007/s00330-023-10127-y. Epub 2023 Aug 18. Eur Radiol. 2024. PMID: 37594523 Free PMC article.
References
-
- Ponikowski P, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016;18:891–975. doi: 10.1002/ejhf.592. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
