

Cervical Spine Evaluation in Pediatric Trauma: A Review and an Update of Current Concepts
- PMID: 30237606
- PMCID: PMC6142799
- DOI: 10.4103/ortho.IJOrtho_607_17
Cervical Spine Evaluation in Pediatric Trauma: A Review and an Update of Current Concepts
Abstract
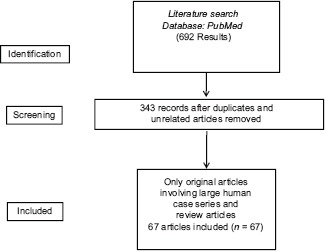
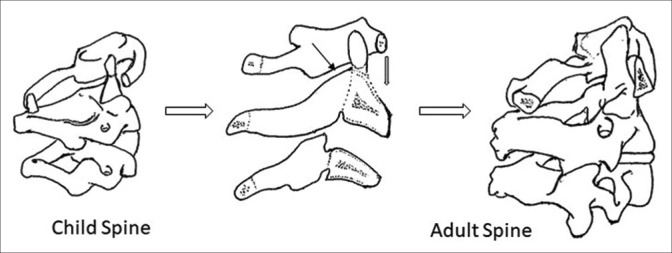
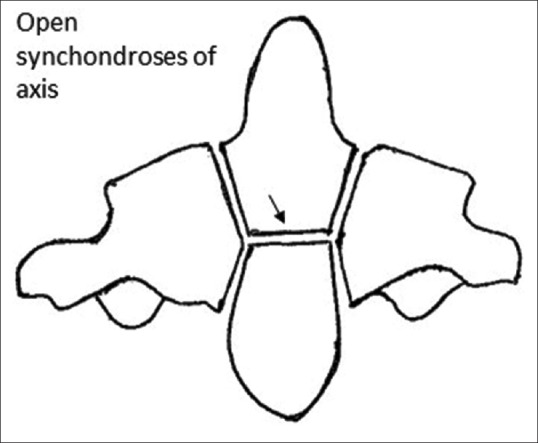
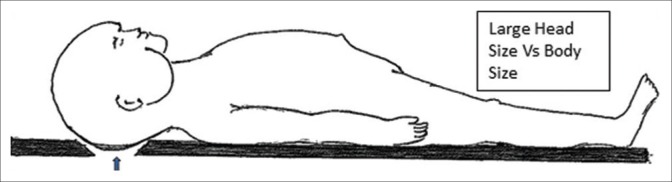
The clinical presentation and diagnostic workup in pediatric cervical spine injuries (CSI) are different from adults owing to the unique anatomy and relative immaturity. The current article reviews the existing literature regarding the uniqueness of these injuries and discusses the current guidelines of radiological evaluation. A PubMed search was conducted using keywords "paediatric cervical spine injuries" or "paediatric cervical spine trauma." Six hundred and ninety two articles were available in total. Three hundred and forty three articles were considered for the review after eliminating unrelated and duplicate articles. Further screening was performed and 67 articles (original articles and review articles only) related to pediatric CSI were finally included. All articles were reviewed for details regarding epidemiology, injury patterns, anatomic considerations, clinical, and radiological evaluation protocols. CSIs are the most common level (60%-80%) for pediatric Spinal Injuries (SI). Children suffer from atlantoaxial injuries 2.5 times more often than adults. Children's unique anatomical features (large head size and highly flexible spine) predispose them to such a peculiar presentation. The role of National Emergency X-Ray Utilization Study, United State (NEXUS) and Canadian Cervical Spine Rule criteria in excluding pediatric cervical injury is questionable but cannot be ruled out completely. The minimum radiological examination includes 2- or 3-view cervical X-rays (anteroposterior, lateral ± open-mouth odontoid views). Additional radiological evaluations, including computerized tomography (CT) and magnetic resonance imaging (MRI) are obtained in situations of abnormal physical examination, abnormal X-rays, inability to obtain adequate X-rays, or to assess cord/soft-tissue status. The clinical criteria for cervical spine injury clearance can generally be applied to children older than 2 years of age. Nevertheless, adequate caution should be exercised before applying these rules in younger children. Initial radiographic investigation should be always adequate plain radiographs of cervical spine. CT and MRI scans should only be performed in an appropriate group of pediatric patients.
Keywords: Anatomical features; Clinical Decision Rules; Pediatrics; anatomy; cervical vertebrae; pediatric cervical spine injuries; spinal cord injuries; spinal cord injury without radiological anomaly.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Cirak B, Ziegfeld S, Knight VM, Chang D, Avellino AM, Paidas CN, et al. Spinal injuries in children. J Pediatr Surg. 2004;39:607–12. - PubMed
-
- McGrory BJ, Klassen RA, Chao EY, Staeheli JW, Weaver AL. Acute fractures and dislocations of the cervical spine in children and adolescents. J Bone Joint Surg Am. 1993;75:988–95. - PubMed
-
- Mathur N, Jain S, Kumar N, Srivastava A, Purohit N, Patni A, et al. Spinal cord injury: Scenario in an Indian state. Spinal Cord. 2015;53:349–52. - PubMed
-
- Booth TN. Cervical spine evaluation in pediatric trauma. AJR Am J Roentgenol. 2012;198:W417–25. - PubMed
-
- Hamilton MG, Myles ST. Pediatric spinal injury: Review of 61 deaths. J Neurosurg. 1992;77:705–8. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources