

Factors Responsible for Redisplacement of Pediatric Forearm Fractures Treated by Closed Reduction and Cast: Role of casting indices and three point index
- PMID: 30237612
- PMCID: PMC6142794
- DOI: 10.4103/ortho.IJOrtho_382_17
Factors Responsible for Redisplacement of Pediatric Forearm Fractures Treated by Closed Reduction and Cast: Role of casting indices and three point index
Abstract
Background: Pediatric forearm fractures are still considered an enigma in view of their propensity to redisplace in cast. The redisplacement may be a potential cause for malalignment. We prospectively analyzed the role of risk factors and above casting indices in predicting significant redisplacement of pediatric forearm fractures treated by closed reduction and cast.
Materials and methods: 113 patients of age range 2-13 years with displaced forearm fractures, treated by closed reduction and cast were included in this prospective study. Prereduction and postreduction angulation, translation, and shortening were noted. In addition, for distal metaphyseal fractures, obliquity angle was noted. In postreduction X-ray, apart from fracture variables, casting indices were also noted (cast index [CI] for all patients with three-point index [TPI] and second metacarpal radius angle in addition for distal metaphyseal fractures). In 2nd week, X-rays were again obtained to check for significant redisplacement. These patients were managed with remanipulation and casting or were operated if remanipulation failed. Comparison of various risk factors was made between patients with significant redisplacement and those which were acceptably reduced. A subgroup analysis of patients with distal metaphyseal fractures was done.
Results: Thirteen (11.5%) patients had significant redisplacement; all of them required remanipulation. No association with respect to age, sex, level of fracture, side of injury, surgeon's experience, number of bones fractured, and injury to definitive cast interval was seen. The presence of complete displacement in any of the plane in either of the bones was seen to be highly significant predictor of redisplacement (P < 0.001). Postreduction angulation more than 10° in any plane in either of the bone and fracture obliquity angle in distal metaphyseal fracture also had a highly significant association with redisplacement. There was a significant difference in the mean values of all three casting indices assessed. TPI was the most sensitive casting index (87.5%).
Conclusions: Conservative management with aim of anatomical reduction, especially in patients with complete displacement, should be the approach of choice in closed pediatric forearm fractures. Casting indices are good markers of quality of cast.
Keywords: Cast index; Pediatrics; bone; casting indices; closed reduction and cast; forearm; fracture; pediatric forearm fractures; plaster cast; redisplacement; second metacarpal radius angle; three-point index.
Conflict of interest statement
There are no conflicts of interest.
Figures
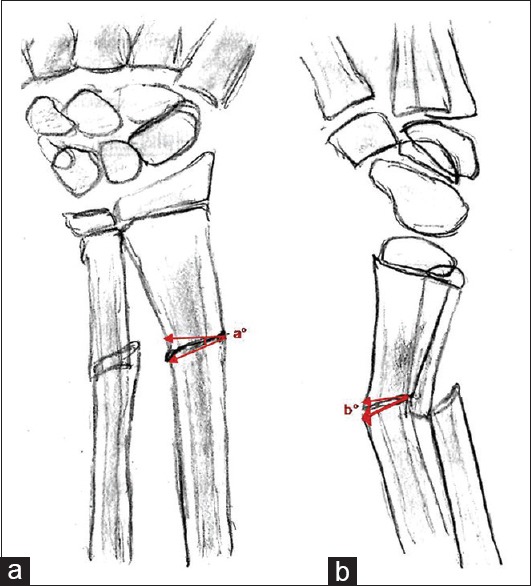



 TPI = ([a + b + c]/d) + ([e + f + g]/h). Cut off value <0.8. TPI = Three point index, AP = Anteroposterior
TPI = ([a + b + c]/d) + ([e + f + g]/h). Cut off value <0.8. TPI = Three point index, AP = Anteroposterior


Similar articles
-
Risk factors for fracture redisplacement after reduction and cast immobilization of displaced distal radius fractures in children: a meta-analysis.Eur J Trauma Emerg Surg. 2020 Aug;46(4):789-800. doi: 10.1007/s00068-019-01227-w. Epub 2019 Sep 9. Eur J Trauma Emerg Surg. 2020. PMID: 31502066 Free PMC article. Review.
-
Do We Need to Stabilize All Reduced Metaphyseal Both-bone Forearm Fractures in Children with K-wires?Clin Orthop Relat Res. 2022 Feb 1;480(2):395-404. doi: 10.1097/CORR.0000000000001980. Clin Orthop Relat Res. 2022. PMID: 34533477 Free PMC article.
-
Risk factors for redisplacement of pediatric distal forearm and distal radius fractures.J Pediatr Orthop. 2012 Oct-Nov;32(7):687-92. doi: 10.1097/BPO.0b013e31824b7525. J Pediatr Orthop. 2012. PMID: 22955532
-
Three-point index in predicting redisplacement of extra-articular distal radial fractures in adults.Injury. 2010 Feb;41(2):197-203. doi: 10.1016/j.injury.2009.08.021. Epub 2009 Sep 26. Injury. 2010. PMID: 19782974
-
Paediatric forearm and distal radius fractures: risk factors and re-displacement--role of casting indices.Int Orthop. 2010 Mar;34(3):407-12. doi: 10.1007/s00264-009-0904-0. Int Orthop. 2010. PMID: 19916008 Free PMC article. Review.
Cited by
-
The influence of casting techniques on the redisplacement risk of reduced distal radius fractures in adults.Arch Orthop Trauma Surg. 2025 May 31;145(1):326. doi: 10.1007/s00402-025-05910-z. Arch Orthop Trauma Surg. 2025. PMID: 40448857 Free PMC article.
-
Risk factors for fracture redisplacement after reduction and cast immobilization of displaced distal radius fractures in children: a meta-analysis.Eur J Trauma Emerg Surg. 2020 Aug;46(4):789-800. doi: 10.1007/s00068-019-01227-w. Epub 2019 Sep 9. Eur J Trauma Emerg Surg. 2020. PMID: 31502066 Free PMC article. Review.
-
Short and long-arm fiberglass cast immobilization for displaced distal forearm fractures in children: a randomized controlled trial.Int Orthop. 2021 Mar;45(3):759-768. doi: 10.1007/s00264-020-04800-w. Epub 2020 Sep 17. Int Orthop. 2021. PMID: 32940750 Free PMC article. Clinical Trial.
-
Functional Outcome of Closed Reduction and Extension Casting in Forearm Fractures in Children.Cureus. 2022 Feb 19;14(2):e22389. doi: 10.7759/cureus.22389. eCollection 2022 Feb. Cureus. 2022. PMID: 35371711 Free PMC article.
-
Incidence and risk factors for redisplacement after closed reduction and instant rigid cast immobilization for paediatric distal radius fractures: a case control study.J Orthop Surg Res. 2020 Apr 9;15(1):140. doi: 10.1186/s13018-020-01672-z. J Orthop Surg Res. 2020. PMID: 32272949 Free PMC article.
References
-
- Bohm ER, Bubbar V, Yong Hing K, Dzus A. Above and below-the-elbow plaster casts for distal forearm fractures in children. A randomized controlled trial. J Bone Joint Surg Am. 2006;88:1–8. - PubMed
-
- Webb GR, Galpin RD, Armstrong DG. Comparison of short and long arm plaster casts for displaced fractures in the distal third of the forearm in children. J Bone Joint Surg Am. 2006;88:9–1. - PubMed
-
- Proctor MT, Moore DJ, Paterson JM. Redisplacement after manipulation of distal radial fractures in children. J Bone Joint Surg Br. 1993;75:453–4. - PubMed
-
- Zamzam MM, Khoshhal KI. Displaced fracture of the distal radius in children: Factors responsible for redisplacement after closed reduction. J Bone Joint Surg Br. 2005;87:841–3. - PubMed
-
- Jones K, Weiner DS. The management of forearm fractures in children: A plea for conservatism. J Pediatr Orthop. 1999;19:811–5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous