

Clinical and Radiographic Outcomes of Pediatric Radial Head Fractures
- PMID: 30237615
- PMCID: PMC6142804
- DOI: 10.4103/ortho.IJOrtho_602_17
Clinical and Radiographic Outcomes of Pediatric Radial Head Fractures
Abstract
Background: The treatment of pediatric radial head fracture (RHF) is controversial, and the outcome is unpredictable. We aimed to evaluate the long term clinical and radiographic outcomes of patients with pediatric RHF.
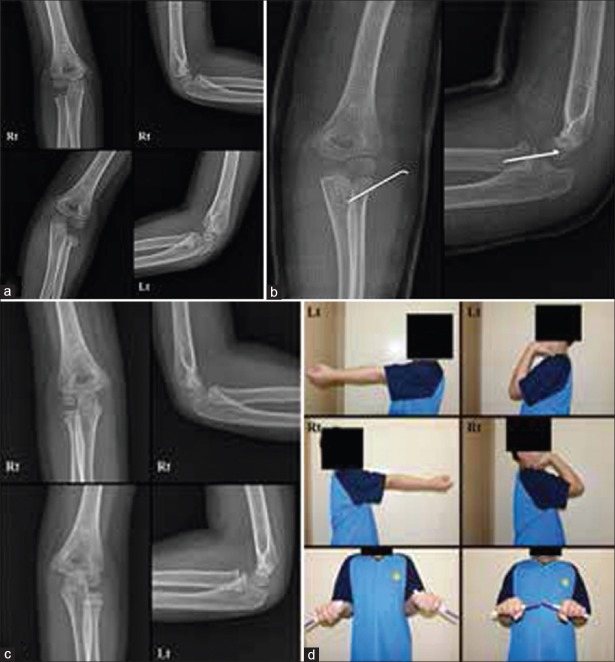
Materials and methods: 24 patients with pediatric RHFs operated between January 2004 and 2012 were included in this retrospective study. 17 patients had extra articular radial head (EARH) fractures and 7 had intraarticular radial head (IARH) fractures. The Mayo Elbow Performance Score (MEPS), Tibone and Stoltz classification, range of motion (ROM), and carrying angle (CA) were evaluated. The radial head diameter (RHD) and radial head height (RHH), neck shaft angle (NSA), and distance from the radial head to the radial tuberosity (RHRT) were measured and compared with the other side in simple anteroposterior views of elbow radiographs.
Results: At the last followup, the mean MEPS was 100 and 97.9 in groups EARH and IARH, respectively. There were no clinically and radiographically significant differences between the groups. The injured elbows showed smaller ROMs than the uninjured elbows in flexion, supination, and pronation with statistically significant differences. However, the injured elbows showed larger extension ranges than the uninjured elbows with a statistical significance (all P = 0.000). CA, RHD, and RHH were higher in the injured elbows than in the uninjured elbows with statistically significant differences (P = 0.006, 0.000, and 0.011) However, NSA and RHRT of both elbows were similar, with no statistically significant difference (P = 0.810 and 0.752).
Conclusion: All patients with pediatric RHF were satisfied with the long term clinical results. The injured elbows showed restricted ROMs compared with the uninjured elbows; however, the extension range increased.
Keywords: Child; Pediatrics; elbow; fracture; prognosis; radius; range of motion.
Conflict of interest statement
There are no conflicts of interest.
Figures



Similar articles
-
Long-term results of radial head resection following isolated radial head fractures in patients younger than forty years old.J Bone Joint Surg Am. 2010 Mar;92(3):558-66. doi: 10.2106/JBJS.I.00332. J Bone Joint Surg Am. 2010. PMID: 20194313
-
Outcome following excision of the radial head in children with open physes for impaired elbow motion.J Shoulder Elbow Surg. 2019 Mar;28(3):525-529. doi: 10.1016/j.jse.2018.08.045. Epub 2018 Nov 27. J Shoulder Elbow Surg. 2019. PMID: 30502032
-
Intra-articular Radial Head Fractures In the Skeletally Immature Patient: Complications and Management.J Pediatr Orthop. 2015 Jul-Aug;35(5):443-8. doi: 10.1097/BPO.0000000000000302. J Pediatr Orthop. 2015. PMID: 25171672
-
Natural history of unreduced Gartland type-II supracondylar fractures of the humerus in children: a two to thirteen-year follow-up study.J Bone Joint Surg Am. 2013 Jan 2;95(1):28-34. doi: 10.2106/jbjs.l.00132. J Bone Joint Surg Am. 2013. PMID: 23405411
-
Is it really necessary to restore radial anatomic parameters after distal radius fractures?Injury. 2014 Dec;45 Suppl 6:S21-6. doi: 10.1016/j.injury.2014.10.018. Epub 2014 Oct 27. Injury. 2014. PMID: 25457314 Review.
Cited by
-
Let's Give Our Best to the Children: The Pediatric Trauma Symposium.Indian J Orthop. 2018 Sep-Oct;52(5):447-448. doi: 10.4103/ortho.IJOrtho_376_18. Indian J Orthop. 2018. PMID: 30237600 Free PMC article. No abstract available.
-
The Presence of Associated Injuries in Pediatric Radial Neck Fractures: A Systematic Review of the Literature and Meta-Analysis of Pooled Individual Patient Data.Children (Basel). 2025 Feb 27;12(3):300. doi: 10.3390/children12030300. Children (Basel). 2025. PMID: 40150584 Free PMC article. Review.
References
-
- O’Brien PI. Injuries involving the proximal radial epiphysis. Clin Orthop Relat Res. 1965;41:51–8. - PubMed
-
- Jeffery CC. Fractures of the head of the radius in children. J Bone Joint Surg Br. 1950;32-B:314–24. - PubMed
-
- D’souza S, Vaishya R, Klenerman L. Management of radial neck fractures in children: A retrospective analysis of one hundred patients. J Pediatr Orthop. 1993;13:232–8. - PubMed
-
- Henrikson B. Isolated fractures of the proximal end of the radius in children epidemiology, treatment and prognosis. Acta Orthop Scand. 1969;40:246–60. - PubMed
-
- Gaston SR, Smith FM, Baab OD. Epiphyseal injuries of the radial head and neck. Am J Surg. 1953;85:266–76. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources