

Isolated Subtalar Arthrodesis
- PMID: 30237922
- PMCID: PMC6145612
- DOI: 10.2106/JBJS.ST.15.00065
Isolated Subtalar Arthrodesis
Abstract
Introduction: An isolated subtalar arthrodesis through a sinus tarsi approach with cannulated screw fixation is safe, reproducible, and effective for specific hindfoot pathology in adults.
Step 1 preoperative planning: Perform a comprehensive clinical and radiographic assessment.
Step 2 patient positioning: Position the patient supine on the operating table with a bump under the ipsilateral hip, to internally rotate the involved leg.
Step 3 incision: Mark a longitudinal incision from just inferior to the tip of the lateral malleolus and extending toward the base of the 4th metatarsal.
Step 4 approach: Expose the subtalar joint by reflecting the extensor digitorum brevis and protecting the peroneal tendons.
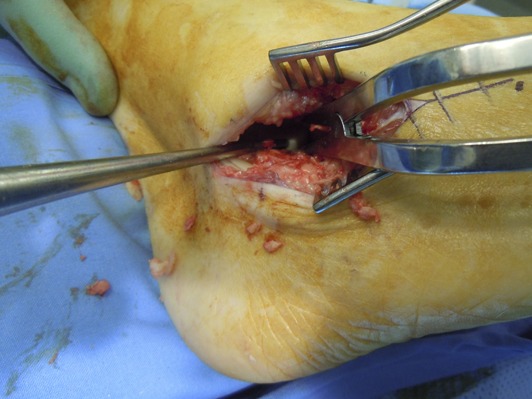
Step 5 joint preparation: Meticulously prepare the subtalar joint using osteotomes and curets down to healthy bleeding subchondral bone.
Step 6 reduction and fixation: Reduce the subtalar joint into 5° of valgus and fix it with cannulated screws.
Step 7 wound closure: Meticulously close the wound in layers and place the lower leg in a well-padded plaster back slab with the ankle in a neutral position.
Step 8 postoperative care: The operatively treated leg is kept immobilized and non-weight-bearing for the first 6 weeks.
Results: Numerous retrospective articles have reported high fusion rates and good functional outcomes after isolated subtalar arthrodesis, for all indications.
Figures
























References
-
- Greisberg J, Sangeorzan B. Hindfoot arthrodesis. J Am Acad Orthop Surg. 2007. January;15(1):65-71. - PubMed
-
- Mann RA. Arthrodesis of the foot and ankle. In: Coughlin MJ, Mann RA, Saltzman CL, editors. Surgery of the foot and ankle. 8th ed Philadelphia: Elsevier Health; 2007. p 1087-123.
-
- Astion DJ, Deland JT, Otis JC, Kenneally S. Motion of the hindfoot after simulated arthrodesis. J Bone Joint Surg Am. 1997. February;79(2):241-6. - PubMed
-
- Roster B, Kreulen C, Giza E. Subtalar joint arthrodesis: open and arthroscopic indications and surgical techniques. Foot Ankle Clin. 2015. June;20(2):319-34. Epub 2015 Apr 11. - PubMed
-
- Hentges MJ, Gesheff MG, Lamm BM. Realignment subtalar joint arthrodesis. J Foot Ankle Surg. 2016. Jan-Feb;55(1):16-21. Epub 2015 May 28. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources