

Autologous Chondrocyte Implantation
- PMID: 30237933
- PMCID: PMC6145632
- DOI: 10.2106/JBJS.ST.16.00018
Autologous Chondrocyte Implantation
Abstract
Introduction: Autologous chondrocyte implantation (ACI) for the treatment of articular cartilage lesions of the knee joint provides successful and durable long-term outcomes.
Step 1 preoperative planning video 1: Obtain standing radiographs and magnetic resonance imaging (MRI) scans to identify all associated abnormalities (background factors).
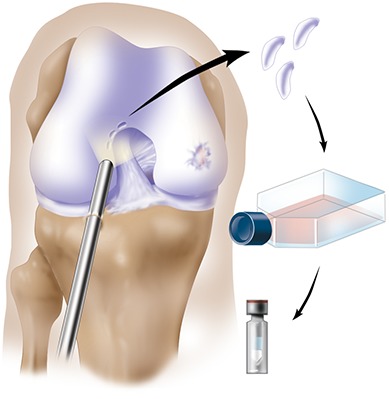
Step 2 arthroscopic assessment and cartilage biopsy video 2: Evaluate the knee joint systematically and harvest cartilage tissue from the non-weight-bearing area.
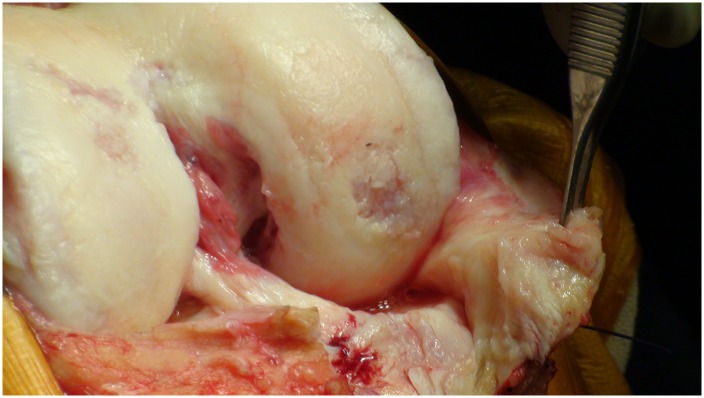
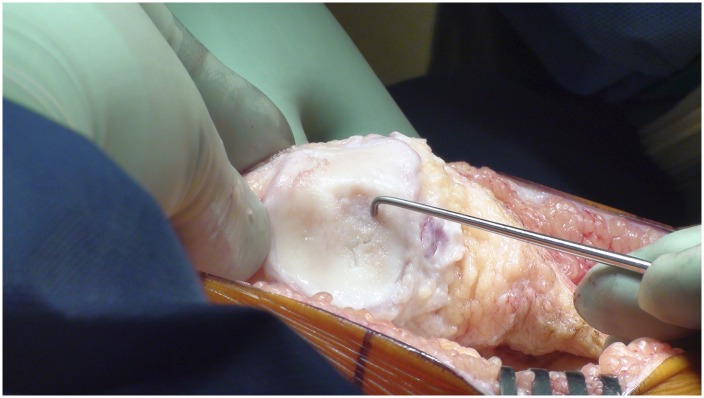
Step 3 make the incision for the arthrotomy video 3: Use a medial or lateral parapatellar arthrotomy and expose the lesion adequately.
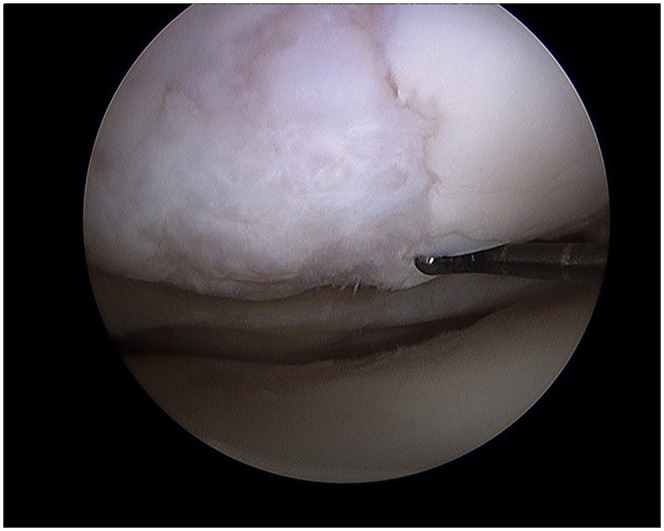
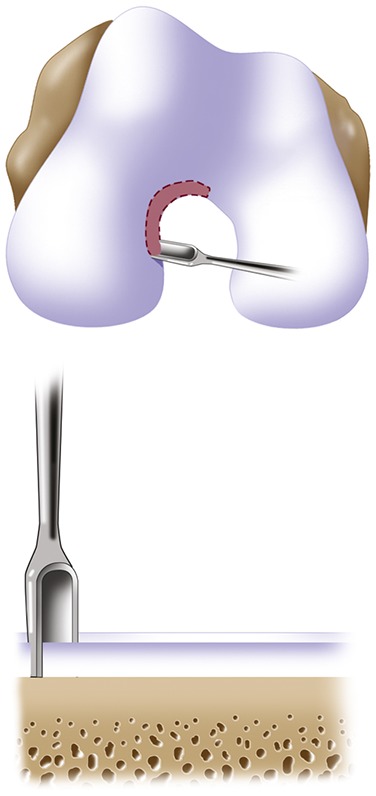
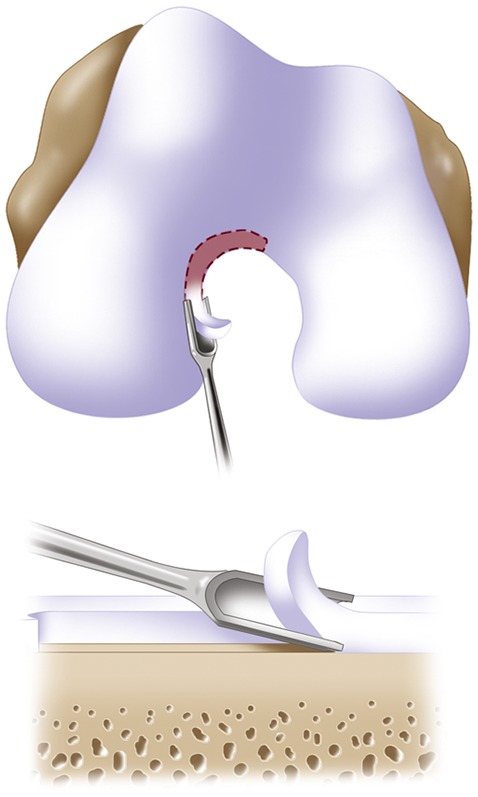
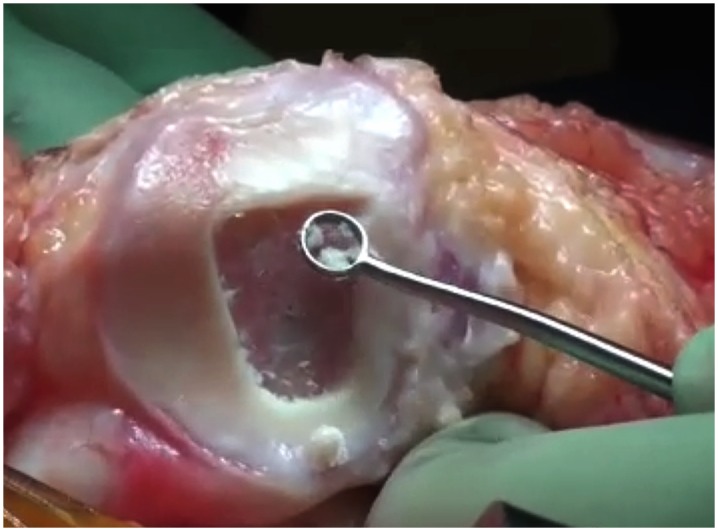
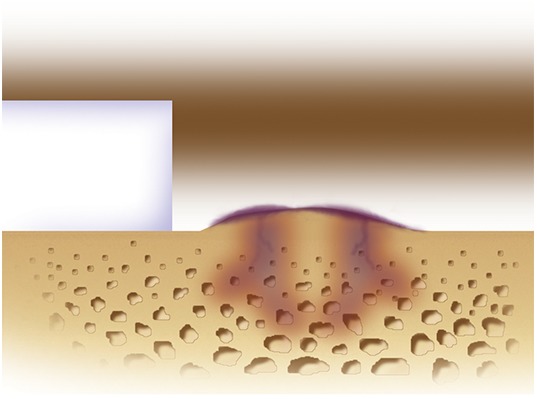
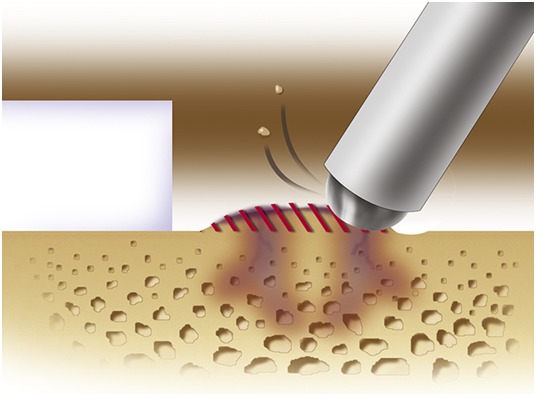
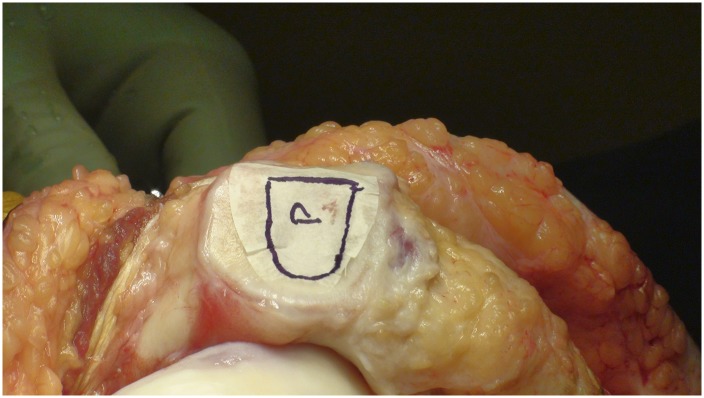
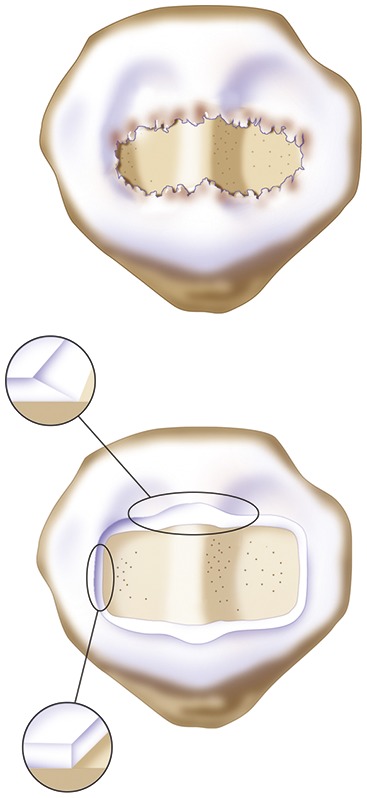
Step 4 prepare the defect video 4: Debride all fissured and unstable articular cartilage surrounding the full-thickness chondral injury down to healthy contained cartilage.
Step 5 address associated abnormalities: Address associated abnormalities (predisposing background factors) to optimize recovery and a successful outcome.
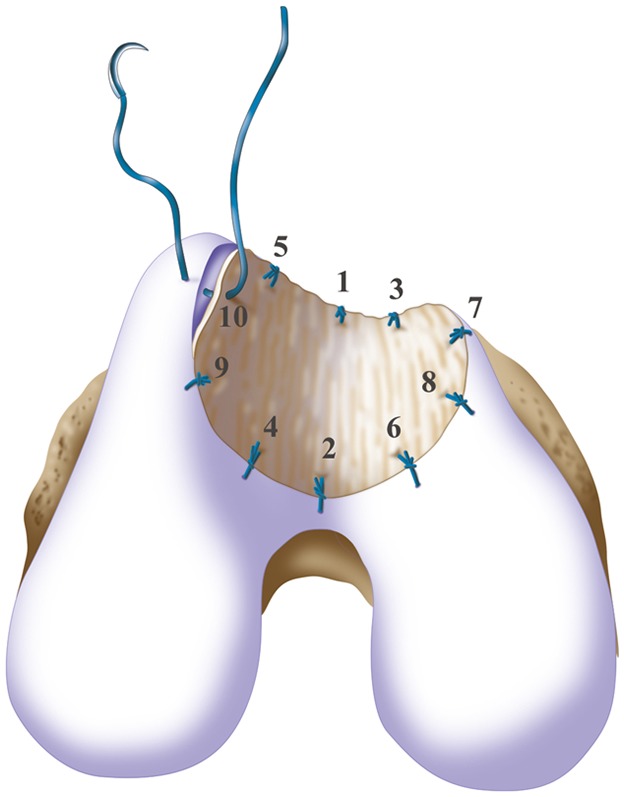
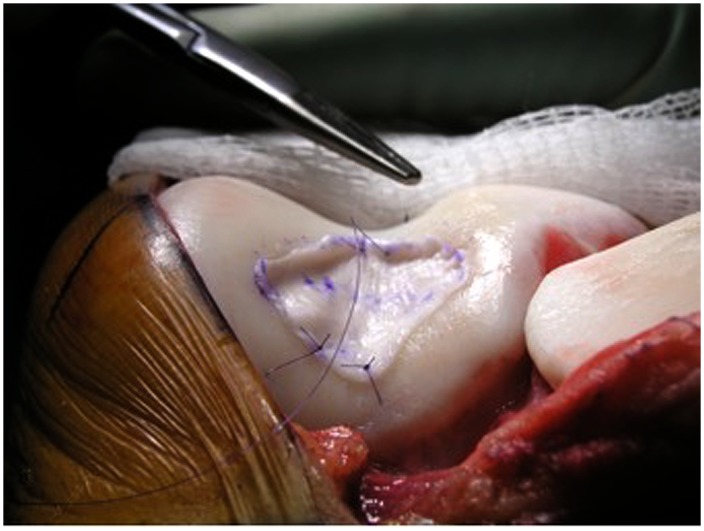
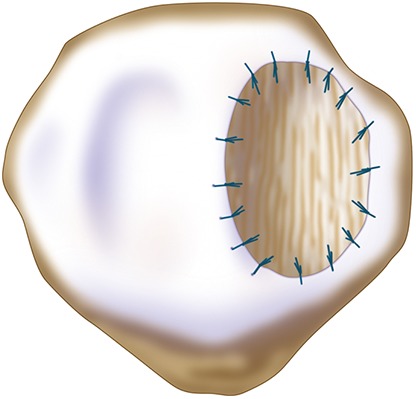
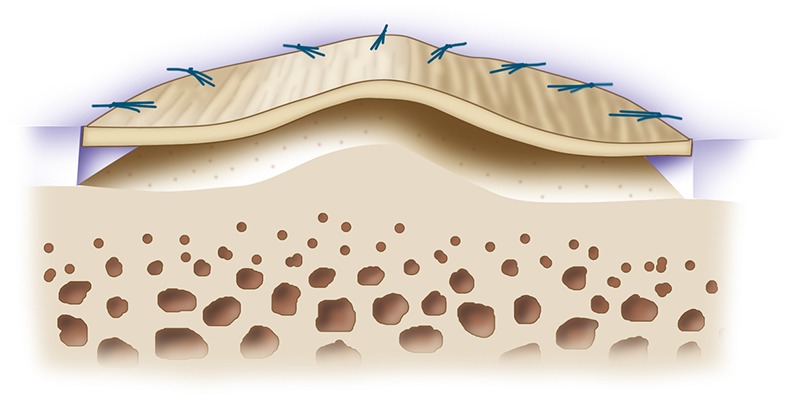
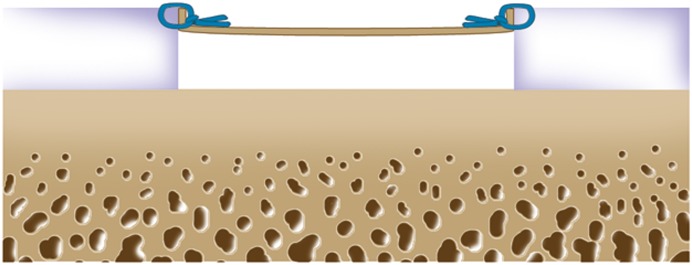
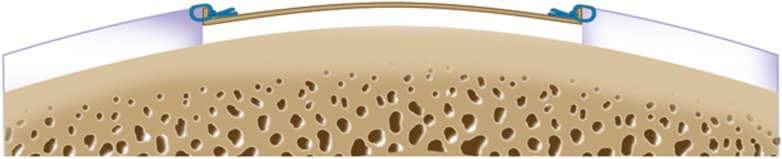
Step 6 prepare and fix the collagen membranes video 5: Orient the membrane patch with the rough surface to the subchondral bone and the smooth surface toward the articular surface; then sew it, tying the sutures knots on the membrane and not the cartilage, to tension it adequately throughout the entire defect.
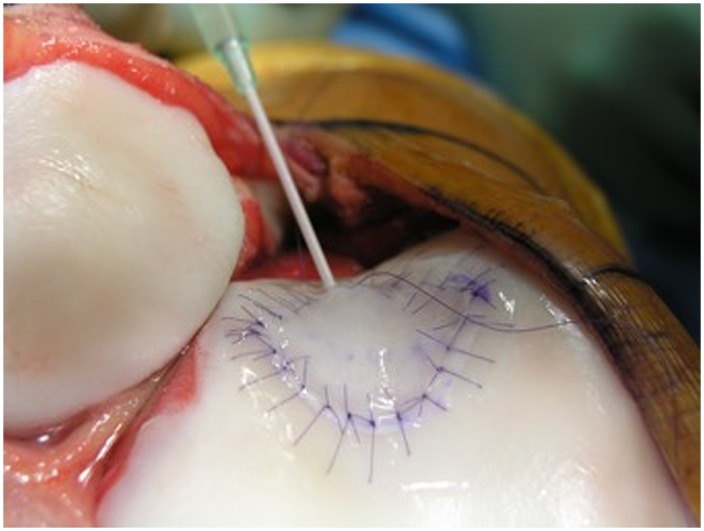
Step 7 chondrocyte implantation video 6: Gently deliver the cells and fill the defect.
Step 8 postoperative care: (1) Initiate range-of-motion exercises to enhance chondrocyte regeneration and decrease the likelihood of intra-articular adhesion, (2) protect the graft from loading for 6 to 12 weeks after surgery to prevent graft overload and central degeneration or delamination of the graft, and (3) initiate isometric muscle exercises to regain muscle tone and prevent atrophy.
Results: ACI provided durable outcomes in 210 patients followed prospectively for 10 to 17 years after treatment with the first-generation ACI-periosteum technique6.
Figures


References
-
- Brittberg M, Lindahl A, Nilsson A, Ohlsson C, Isaksson O, Peterson L. Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med. 1994. October 6;331(14):889-95. - PubMed
-
- Pavesio A, Abatangelo G, Borrione A, Brocchetta D, Hollander AP, Kon E, Torasso F, Zanasi S, Marcacci M. Hyaluronan-based scaffolds (Hyalograft C) in the treatment of knee cartilage defects: preliminary clinical findings. Novartis Found Symp. 2003;249:203-17; discussion 229-33, 234-8, 239-41. - PubMed
-
- Bartlett W, Skinner JA, Gooding CR, Carrington RW, Flanagan AM, Briggs TW, Bentley G. Autologous chondrocyte implantation versus matrix-induced autologous chondrocyte implantation for osteochondral defects of the knee: a prospective, randomised study. J Bone Joint Surg Br. 2005. May;87(5):640-5. - PubMed
-
- Behrens P, Bitter T, Kurz B, Russlies M. Matrix-associated autologous chondrocyte transplantation/implantation (MACT/MACI)—5-year follow-up. Knee. 2006. June;13(3):194-202. Epub 2006 Apr 24. - PubMed
-
- Schneider U, Rackwitz L, Andereya S, Siebenlist S, Fensky F, Reichert J, Löer I, Barthel T, Rudert M, Nöth U. A prospective multicenter study on the outcome of type I collagen hydrogel-based autologous chondrocyte implantation (CaReS) for the repair of articular cartilage defects in the knee. Am J Sports Med. 2011. December;39(12):2558-65. Epub 2011 Oct 7. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical