

Dermatoscopy of Neoplastic Skin Lesions: Recent Advances, Updates, and Revisions
- PMID: 30238167
- PMCID: PMC6153581
- DOI: 10.1007/s11864-018-0573-6
Dermatoscopy of Neoplastic Skin Lesions: Recent Advances, Updates, and Revisions
Abstract
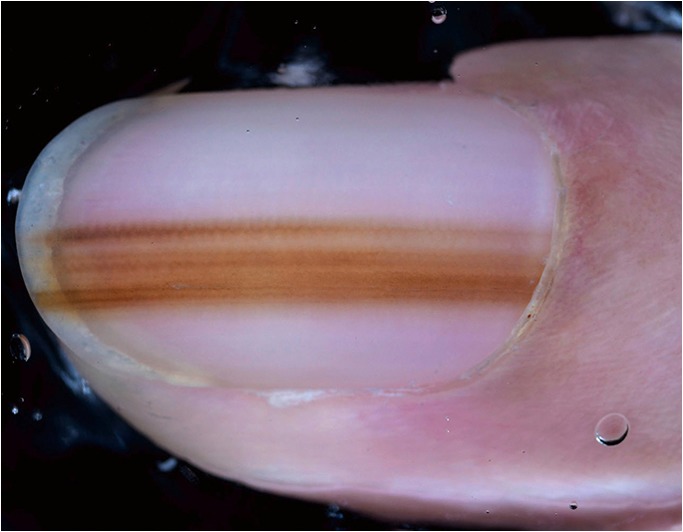
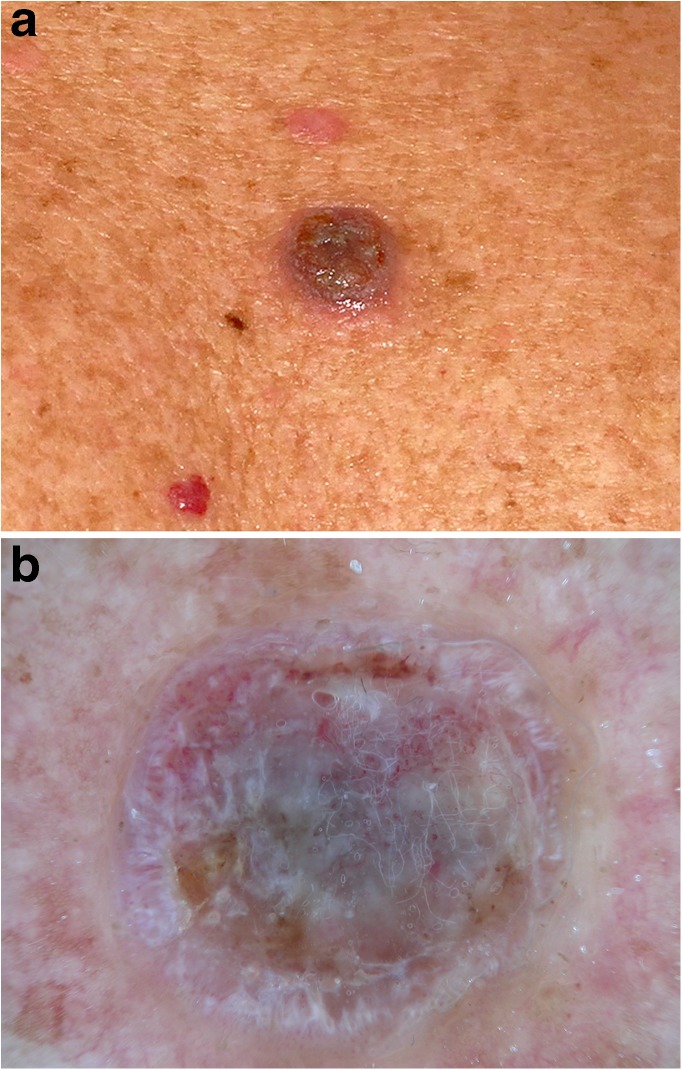
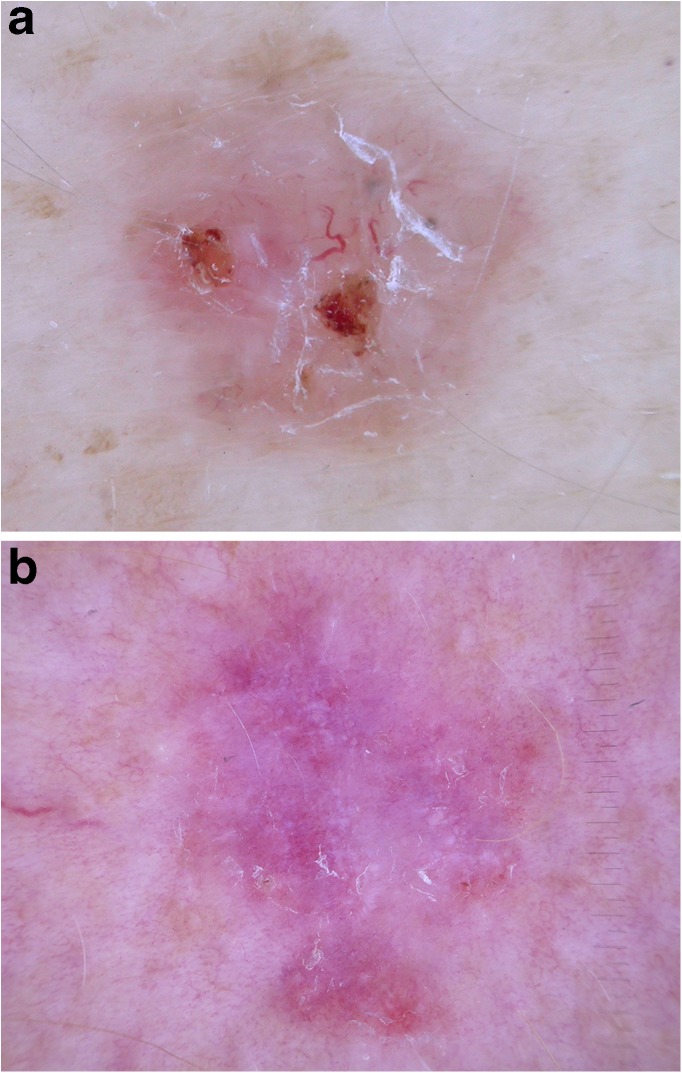
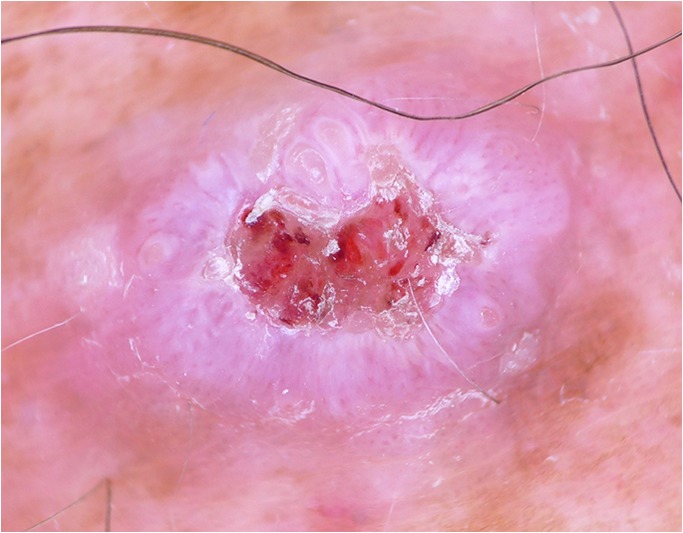
Dermatoscopy (dermoscopy) improves the diagnosis of benign and malignant cutaneous neoplasms in comparison with examination with the unaided eye and should be used routinely for all pigmented and non-pigmented cutaneous neoplasms. It is especially useful for the early stage of melanoma when melanoma-specific criteria are invisible to the unaided eye. Preselection by the unaided eye is therefore not recommended. The increased availability of polarized dermatoscopes, and the extended use of dermatoscopy in non-pigmented lesions led to the discovery of new criteria, and we recommend that lesions should be examined with polarized and non-polarized dermatoscopy. The "chaos and clues algorithm" is a good starting point for beginners because it is easy to use, accurate, and it works for all types of pigmented lesions not only for those melanocytic. Physicians, who use dermatoscopy routinely, should be aware of new clues for acral melanomas, nail matrix melanomas, melanoma in situ, and nodular melanoma. Dermatoscopy should also be used to distinguish between different subtypes of basal cell carcinoma and to discriminate highly from poorly differentiated squamous cell carcinomas to optimize therapy and management of non-melanoma skin cancer. One of the most exciting areas of research is the use of dermatoscopic images for machine learning and automated diagnosis. Convolutional neural networks trained with dermatoscopic images are able to diagnose pigmented lesions with the same accuracy as human experts. We humans should not be afraid of this new and exciting development because it will most likely lead to a peaceful and fruitful coexistence of human experts and decision support systems.
Keywords: Actinic keratosis; Basal cell carcinoma; Dermatoscopy; Dermoscopy; Melanoma; Squamous cell carcinoma.
Conflict of interest statement
Conflict of Interest
Philipp Weber, Philipp Tschandl, Christoph Sinz, and Harald Kittler declare they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Figures
Similar articles
-
Dermatoscopy of non-melanocytic skin tumors.Indian J Dermatol Venereol Leprol. 2011 Jan-Feb;77(1):16-21; quiz 22. doi: 10.4103/0378-6323.74966. Indian J Dermatol Venereol Leprol. 2011. PMID: 21220874 Review.
-
Pink lesions.Dermatol Clin. 2013 Oct;31(4):649-78, ix. doi: 10.1016/j.det.2013.06.005. Dermatol Clin. 2013. PMID: 24075552 Review.
-
Computer-assisted diagnosis techniques (dermoscopy and spectroscopy-based) for diagnosing skin cancer in adults.Cochrane Database Syst Rev. 2018 Dec 4;12(12):CD013186. doi: 10.1002/14651858.CD013186. Cochrane Database Syst Rev. 2018. PMID: 30521691 Free PMC article.
-
Dermoscopy for the family physician.Am Fam Physician. 2013 Oct 1;88(7):441-50. Am Fam Physician. 2013. PMID: 24134084 Review.
-
Dermatoscopy versus Tzanck smear test: a comparison of the value of two tests in the diagnosis of pigmented skin lesions.J Am Acad Dermatol. 2011 Nov;65(5):972-82. doi: 10.1016/j.jaad.2010.08.019. Epub 2011 May 11. J Am Acad Dermatol. 2011. PMID: 21565420 Clinical Trial.
Cited by
-
Attention Cost-Sensitive Deep Learning-Based Approach for Skin Cancer Detection and Classification.Cancers (Basel). 2022 Nov 29;14(23):5872. doi: 10.3390/cancers14235872. Cancers (Basel). 2022. PMID: 36497355 Free PMC article.
-
The "Virtual Biopsy" of Cancerous Lesions in 3D: Non-Invasive Differentiation between Melanoma and Other Lesions Using Vibrational Optical Coherence Tomography.Dermatopathology (Basel). 2021 Dec 13;8(4):539-551. doi: 10.3390/dermatopathology8040058. Dermatopathology (Basel). 2021. PMID: 34940035 Free PMC article.
-
Pathogenesis, Diagnosis and Management of Squamous Cell Carcinoma and Pseudoepithelial Hyperplasia Secondary to Red Ink Tattoo: A Case Series and Review.J Clin Med. 2023 Mar 21;12(6):2424. doi: 10.3390/jcm12062424. J Clin Med. 2023. PMID: 36983424 Free PMC article. Review.
-
Risk factors for actinic keratosis, non-melanoma skin cancer and cutaneous malignant melanoma in persons with and without Parkinson's disease: A cross-sectional study.Skin Health Dis. 2024 Oct 4;4(6):e464. doi: 10.1002/ski2.464. eCollection 2024 Dec. Skin Health Dis. 2024. PMID: 39624738 Free PMC article.
-
Non-Melanoma Skin Cancer Clearance after Medical Treatment Detected with Noninvasive Skin Imaging: A Systematic Review and Meta-Analysis.Cancers (Basel). 2022 Jun 8;14(12):2836. doi: 10.3390/cancers14122836. Cancers (Basel). 2022. PMID: 35740502 Free PMC article. Review.
References
References and Recommended Reading
Papers of particular interest, published recently, have been highlighted as: •• Of major importance
-
- Argenziano G, Soyer HP, Chimenti S, Talamini R, Corona R, Sera F, Binder M, Cerroni L, de Rosa G, Ferrara G, Hofmann-Wellenhof R, Landthaler M, Menzies SW, Pehamberger H, Piccolo D, Rabinovitz HS, Schiffner R, Staibano S, Stolz W, Bartenjev I, Blum A, Braun R, Cabo H, Carli P, de Giorgi V, Fleming MG, Grichnik JM, Grin CM, Halpern AC, Johr R, Katz B, Kenet RO, Kittler H, Kreusch J, Malvehy J, Mazzocchetti G, Oliviero M, zdemir F, Peris K, Perotti R, Perusquia A, Pizzichetta MA, Puig S, Rao B, Rubegni P, Saida T, Scalvenzi M, Seidenari S, Stanganelli I, Tanaka M, Westerhoff K, Wolf IH, Braun-Falco O, Kerl H, Nishikawa T, Wolff K, Kopf AW. Dermoscopy of pigmented skin lesions: results of a consensus meeting via the Internet. J Am Acad Dermatol. 2003;48(5):679–693. doi: 10.1067/mjd.2003.281. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
