

Pathological significance of urinary complement activation in diabetic nephropathy: A full view from the development of the disease
- PMID: 30239170
- PMCID: PMC6497774
- DOI: 10.1111/jdi.12934
Pathological significance of urinary complement activation in diabetic nephropathy: A full view from the development of the disease
Abstract
Aims/introduction: The aim of the present study was to obtain a full view of the changes of urinary complement activation products in the development of diabetic nephropathy and explore their possible significance in the disease process.
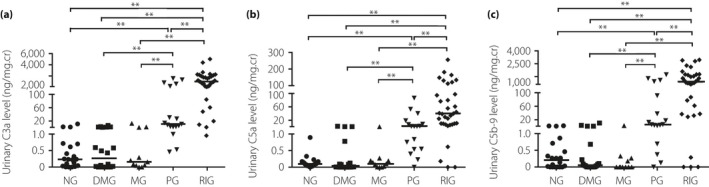
Materials and methods: A total of 62 patients at different stages of diabetic nephropathy, 20 diabetes patients without nephropathy and 20 healthy persons were enrolled. Urinary complement activation products, including C3a, C5a and C5b-9, were measured, and their associations with the progression of the disease were analyzed.
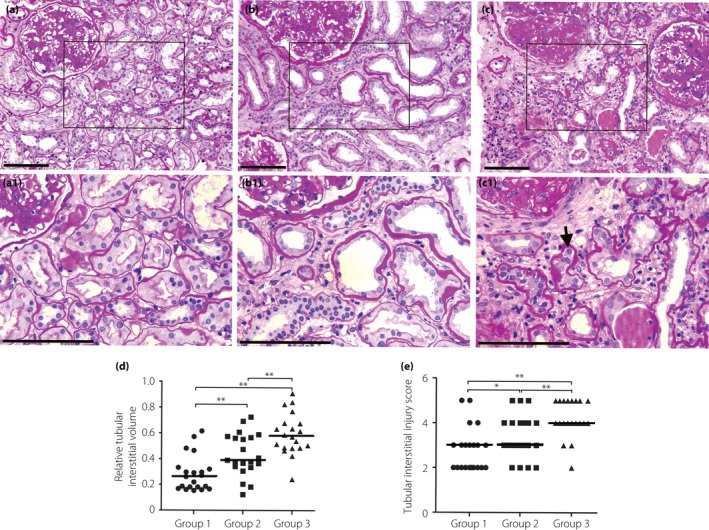
Results: The urinary complement activation products increased markedly since the proteinuria stage, and were parallel with the progression of diabetic nephropathy. More severe renal tubular damage was observed in patients with higher levels of urinary complement activation products. The urinary complement activation products levels correlated closely with renal tubulointerstitial injury score and relative tubular interstitial volume. Multivariate regression analysis showed that elevated urinary complement activation products were independent risk factors for tubular injury in diabetic nephropathy patients.
Conclusions: Urinary complement activation might have a role in renal tubular interstitial injury in patients with diabetic nephropathy, especially in patients at a later stage of the disease.
Keywords: Diabetic nephropathy; Tubular injury; Urinary complement activation products.
© 2018 The Authors. Journal of Diabetes Investigation published by Asian Association for the Study of Diabetes (AASD) and John Wiley & Sons Australia, Ltd.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
