

Increased Relative Abundance of Klebsiella pneumoniae Carbapenemase-producing Klebsiella pneumoniae Within the Gut Microbiota Is Associated With Risk of Bloodstream Infection in Long-term Acute Care Hospital Patients
- PMID: 30239622
- PMCID: PMC6541703
- DOI: 10.1093/cid/ciy796
Increased Relative Abundance of Klebsiella pneumoniae Carbapenemase-producing Klebsiella pneumoniae Within the Gut Microbiota Is Associated With Risk of Bloodstream Infection in Long-term Acute Care Hospital Patients
Abstract
Background: An association between increased relative abundance of specific bacterial taxa in the intestinal microbiota and bacteremia has been reported in some high-risk patient populations.
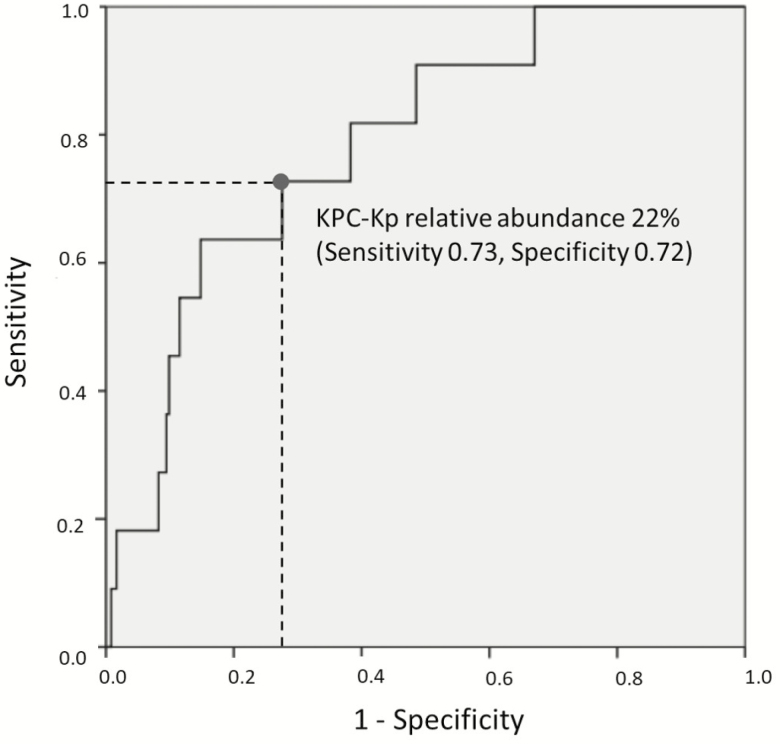
Methods: We collected weekly rectal swab samples from patients at 1 long-term acute care hospital (LTACH) in Chicago from May 2015 to May 2016. Samples positive for Klebsiella pneumoniae carbapenemase-producing Klebsiella pneumoniae (KPC-Kp) by polymerase chain reaction and culture underwent 16S rRNA gene sequence analysis; relative abundance of the operational taxonomic unit containing KPC-Kp was determined. Receiver operator characteristic (ROC) curves were constructed using results from the sample with highest relative abundance of KPC-Kp from each patient admission, excluding samples collected after KPC-Kp bacteremia. Cox regression analysis was performed to evaluate risk factors associated with time to achieve KPC-Kp relative abundance thresholds calculated by ROC curve analysis.
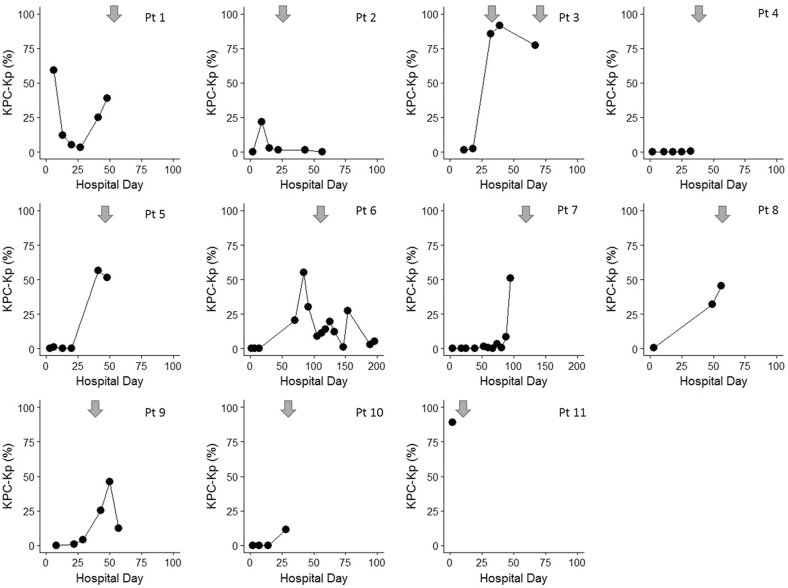
Results: We collected 2319 samples from 562 admissions (506 patients); KPC-Kp colonization was detected in 255 (45.4%) admissions and KPC-Kp bacteremia in 11 (4.3%). A relative abundance cutoff of 22% predicted KPC-Kp bacteremia with sensitivity 73%, specificity 72%, and relative risk 4.2 (P = .01). In a multivariable Cox regression model adjusted for age, Charlson comorbidity index, and medical devices, carbapenem receipt was associated with achieving the 22% relative abundance threshold (P = .044).
Conclusion: Carbapenem receipt was associated with increased hazard for high relative abundance of KPC-Kp in the gut microbiota. Increased relative abundance of KPC-Kp was associated with KPC-Kp bacteremia. Whether bacteremia arose directly from bacterial translocation or indirectly from skin contamination followed by bloodstream invasion remains to be determined.
Keywords: bloodstream infection; carbapenemase-producing Klebsiella pneumoniae; intestinal domination; long-term acute care hospital; microbiome.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- van der Velden WJ, Herbers AH, Netea MG, Blijlevens NM. Mucosal barrier injury, fever and infection in neutropenic patients with cancer: introducing the paradigm febrile mucositis. Br J Haematol 2014; 167:441–52. - PubMed
-
- Balzan S, de Almeida Quadros C, de Cleva R, Zilberstein B, Cecconello I. Bacterial translocation: overview of mechanisms and clinical impact. J Gastroenterol Hepatol 2007; 22:464–71. - PubMed
-
- Wiest R, Garcia-Tsao G. Bacterial translocation (BT) in cirrhosis. Hepatology 2005; 41:422–33. - PubMed
-
- Young VB. The role of the microbiome in human health and disease: an introduction for clinicians. BMJ 2017; 356:j831. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
