

A Revised Diagnostic Classification of Canine Glioma: Towards Validation of the Canine Glioma Patient as a Naturally Occurring Preclinical Model for Human Glioma
- PMID: 30239918
- PMCID: PMC6181180
- DOI: 10.1093/jnen/nly085
A Revised Diagnostic Classification of Canine Glioma: Towards Validation of the Canine Glioma Patient as a Naturally Occurring Preclinical Model for Human Glioma
Abstract
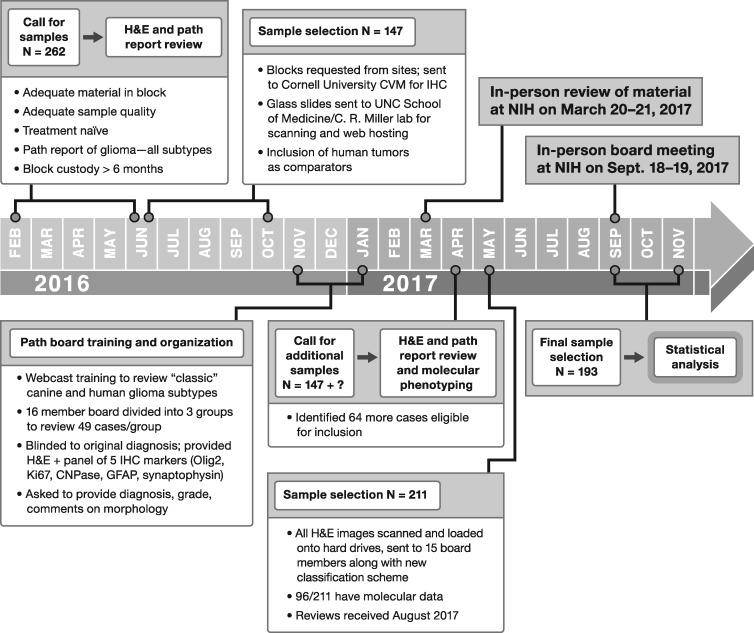
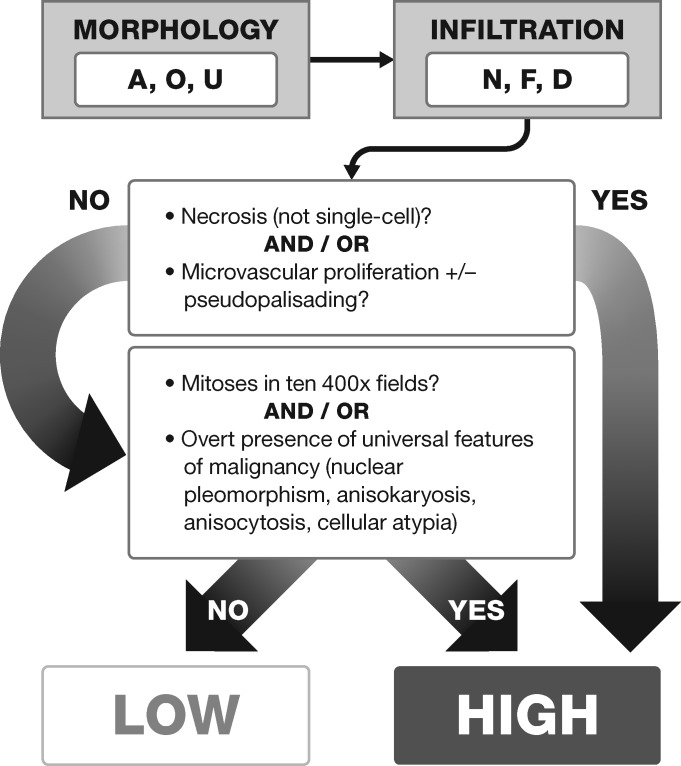
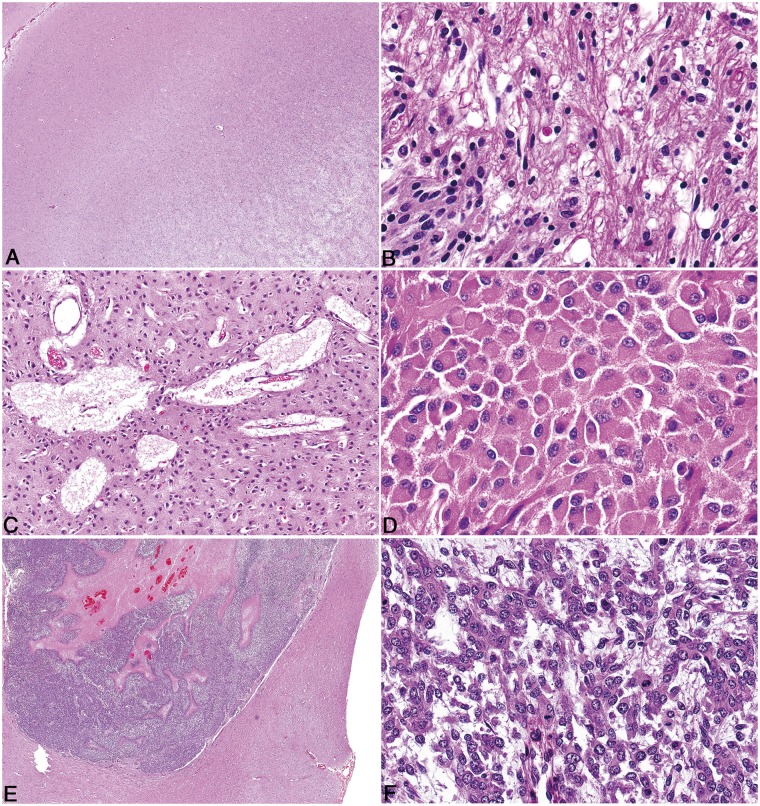
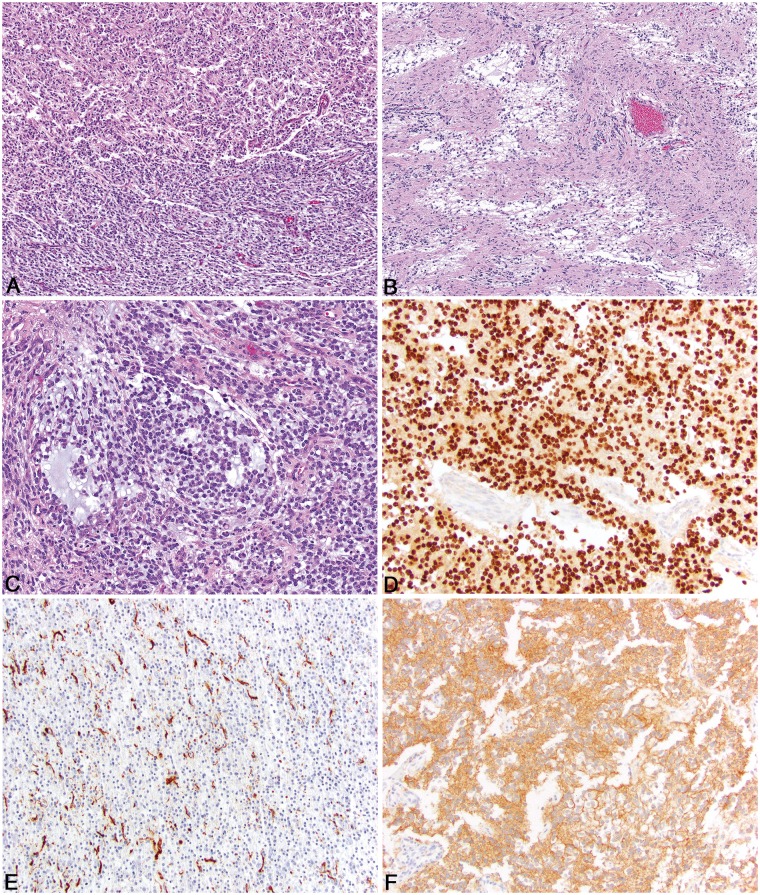
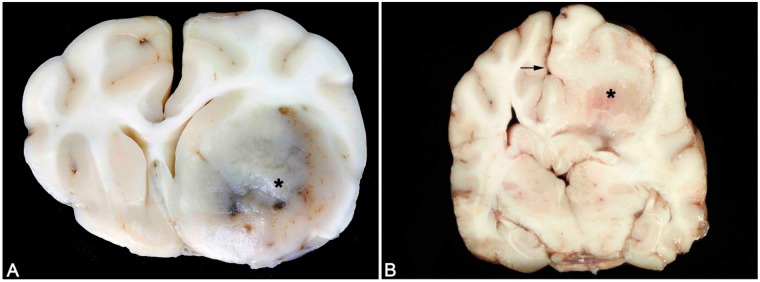
The National Cancer Institute-led multidisciplinary Comparative Brain Tumor Consortium (CBTC) convened a glioma pathology board, comprising both veterinarian and physician neuropathologists, and conducted a comprehensive review of 193 cases of canine glioma. The immediate goal was to improve existing glioma classification methods through creation of a histologic atlas of features, thus yielding greater harmonization of phenotypic characterization. The long-term goal was to support future incorporation of clinical outcomes and genomic data into proposed simplified diagnostic schema, so as to further bridge the worlds of veterinary and physician neuropathology and strengthen validity of the dog as a naturally occurring, translationally relevant animal model of human glioma. All cases were morphologically reclassified according to a new schema devised by the entire board, yielding a majority opinion diagnosis of astrocytoma (43, 22.3%), 19 of which were low-grade and 24 high-grade, and oligodendroglioma (134, 69.4%), 35 of which were low-grade and 99 were high-grade. Sixteen cases (8.3%) could not be classified as oligodendroglioma or astrocytoma based on morphology alone and were designated as undefined gliomas. The simplified classification scheme proposed herein provides a tractable means for future addition of molecular data, and also serves to highlight histologic similarities and differences between human and canine glioma.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
