

Why do ambulance services have different non-transport rates? A national cross sectional study
- PMID: 30240418
- PMCID: PMC6150527
- DOI: 10.1371/journal.pone.0204508
Why do ambulance services have different non-transport rates? A national cross sectional study
Abstract
Background: Some patients calling ambulance services (known as Emergency Medical Services internationally) are not transported to hospital. In England, national ambulance quality indicators show considerable variation in non-transport rates between the ten large regional ambulance services. The aim of this study was to explain variation between ambulance services in two types of non-transport: discharge at scene and telephone advice.
Methods: Mixed model logistic regressions using one month of data (November 2014) from the Computer Aided Despatch systems of the ten large regional ambulance services in England.
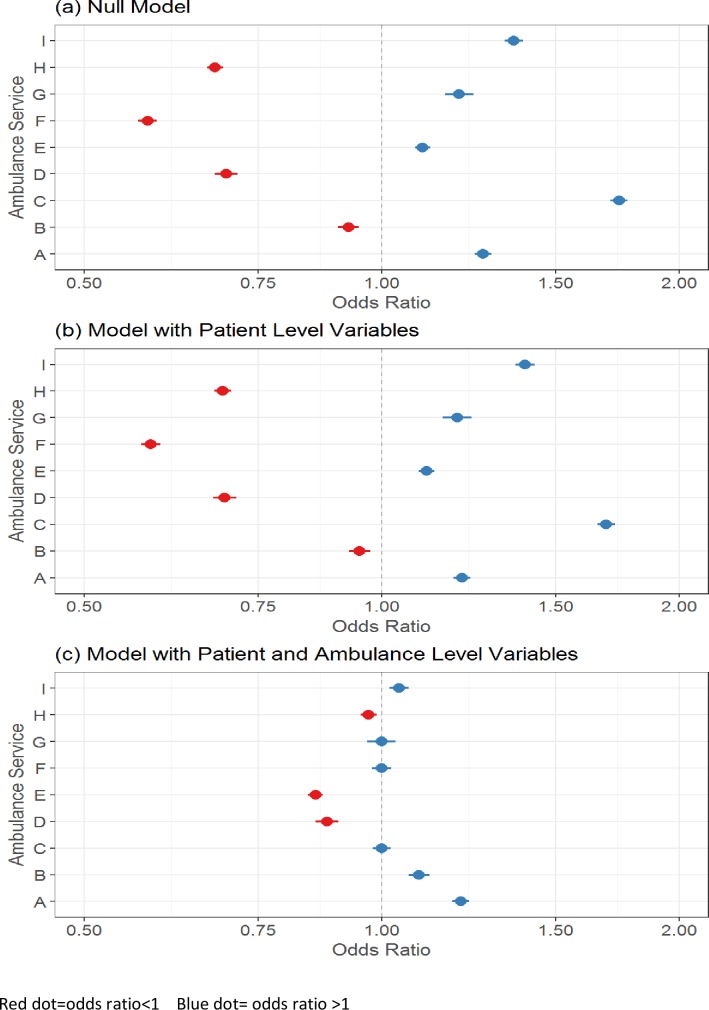
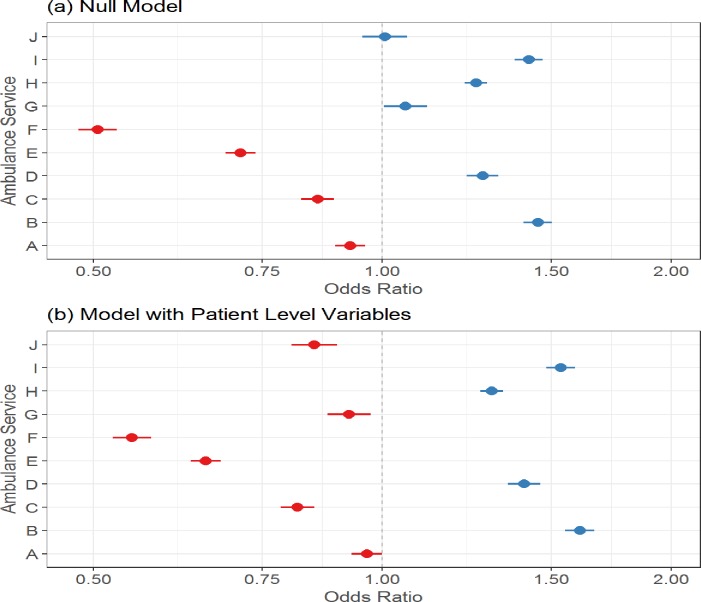
Results: 41% (251 677/615 815) of patients calling ambulance services were not transported to hospital. Most were discharged at scene after attendance by an ambulance (29% n = 182 479) and a small percentage were given telephone advice (7% n = 40 679). Discharge at scene rates varied by patient-level factors e.g. they were higher for elderly patients, where the reason for calling was falls, and for patients attended by paramedics with extended skills. These patient-level factors did not explain variation between ambulance services. After adjustment for patient-level factors, the following ambulance service level factors explained variation in discharge at scene rates: proportion of patients attended by paramedics with extended skills (odds ratio 1.05 (95% CI 1.04, 1.07)), the perception of ambulance service staff that paramedics with extended skills were established and valued within the workforce (odds ratio 1.84 (1.45, 2.33), and the perception of ambulance service staff that senior management viewed non-transport as risky (odds ratio 0.78 (0.63, 0.98)). Variation in telephone advice rates could not be explained.
Conclusions: Variation in discharge at scene rates was explained by differences in workforce configuration and managerial motivation, factors that are largely modifiable by ambulance services.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Alrazeeni DM, Sheikh SA, Mobrad A, Ghamdi MA, Abdulqader N, Gadgab MA, et al. Epidemiology of non-transported emergency medical services calls in Saudi Arabia. Saudi Med J 2016;37(5):575–8. doi: 10.15537/smj.2016.5.13872 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
