

Short-Term Outcomes of Tracheal Resection in The Society of Thoracic Surgeons Database
- PMID: 30240762
- PMCID: PMC6696934
- DOI: 10.1016/j.athoracsur.2018.07.041
Short-Term Outcomes of Tracheal Resection in The Society of Thoracic Surgeons Database
Abstract
Background: Tracheal surgery is uncommon, and most of the published literature consists of single-center series over large periods. Our goal was to perform a national, contemporary analysis to identify predictors of major morbidity and mortality based on indication and surgical approach.
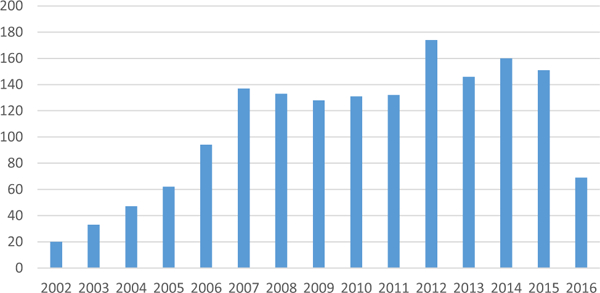
Methods: The Society of Thoracic Surgeons General Thoracic Surgery Database (STS GTSD) was queried for all patients undergoing tracheal resection between 2002 and 2016. We identified 1,617 cases and compared outcomes by indication and approach. We created a multivariable model for a combined end point of mortality or major morbidity. The relationship between volume and outcome was analyzed.
Results: The cervical approach was used 81% of the time, and benign disease was the indication in 75% of cases. Overall 30-day mortality was 1%, and no significant difference was found between the cervical and thoracic approach (1.1% versus 1.6%, p = 0.57) or between benign and malignant indications (1.1% versus 1.5%, p = 0.61). Independent factors associated with morbidity or mortality included thoracic approach, diabetes, and functional status. Centers were divided into those averaging fewer than four resections per year and those performing at least four per year. The low volume (<4) group had a combined morbidity and mortality of 27%, significantly higher than 17% observed among centers with more than four per year (p < 0.0001).
Conclusions: STS GTSD participants perform tracheal resection for benign and malignant disease with low early morbidity and mortality. Higher operative volume is associated with improved outcome. Longer follow-up is needed to confirm airway stability and rate of reoperation.
Copyright © 2018 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Comment in
-
The Tribulation of Tracheal Surgery.Ann Thorac Surg. 2019 Nov;108(5):1586. doi: 10.1016/j.athoracsur.2019.02.037. Epub 2019 Mar 22. Ann Thorac Surg. 2019. PMID: 30910652 No abstract available.
-
Reply.Ann Thorac Surg. 2019 Nov;108(5):1586. doi: 10.1016/j.athoracsur.2019.04.076. Epub 2019 Jun 15. Ann Thorac Surg. 2019. PMID: 31653295 No abstract available.
References
-
- Geffin B, Grillo HC, Cooper JD, Pontoppidan H. Stenosis following tracheostomy for respiratory care. JAMA 1971;216: 1984–8. - PubMed
-
- Grillo HC. The management of tracheal stenosis following assisted respiration. J Thorac Cardiovasc Surg 1969;57: 52–71. - PubMed
-
- Pearson FG, Todd TR, Cooper JD. Experience with primary neoplasms of the trachea and carina. J Thorac Cardiovasc Surg 1984;88:511–8. - PubMed
-
- Macchiarini P, Chapelier A, Lenot B, Cerrina J, Dartevelle P. Laryngotracheal resection and reconstruction for postintubation subglottic stenosis. Lessons learned. Eur J Cardiothorac Surg 1993;7:300–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
