

The impact of HIV on the prevalence of asthma in Uganda: a general population survey
- PMID: 30241519
- PMCID: PMC6151019
- DOI: 10.1186/s12931-018-0898-5
The impact of HIV on the prevalence of asthma in Uganda: a general population survey
Abstract
Background: HIV and asthma are highly prevalent diseases in Africa but few studies have assessed the impact of HIV on asthma prevalence in high HIV burden settings. The objective of this analysis was to compare the prevalence of asthma among persons living with HIV (PLHIV) and those without HIV participating in the Uganda National Asthma Survey (UNAS).
Methods: UNAS was a population-based survey of persons aged ≥12 years. Asthma was diagnosed based on either self-reported current wheeze concurrently or within the prior 12 months; physician diagnosis; or use of asthma medication. HIV was defined based on confidential self-report. We used Poisson regression with robust standard errors to estimate asthma prevalence and the prevalence ratio (PR) for HIV and asthma.
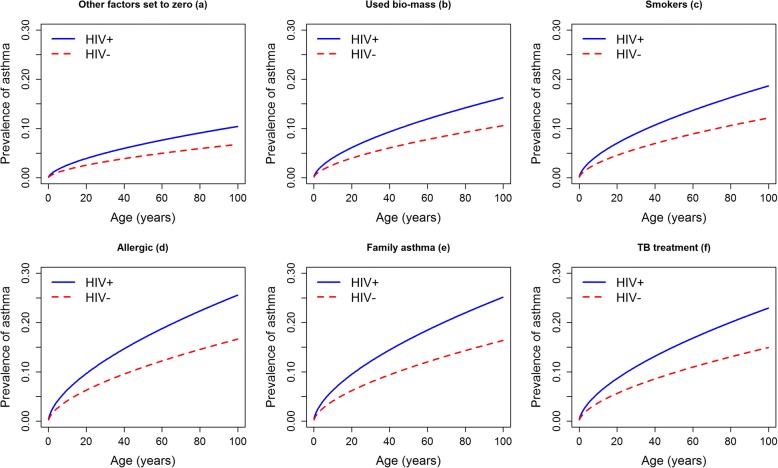
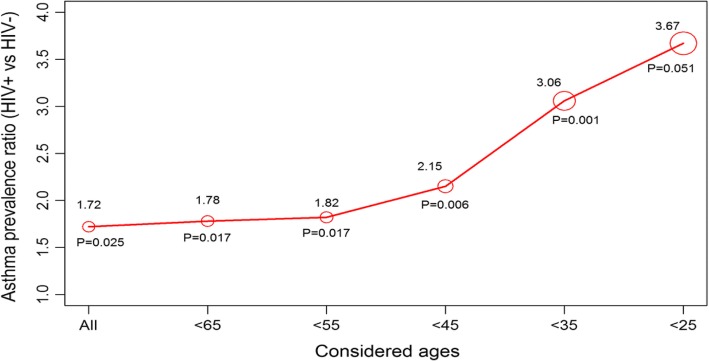
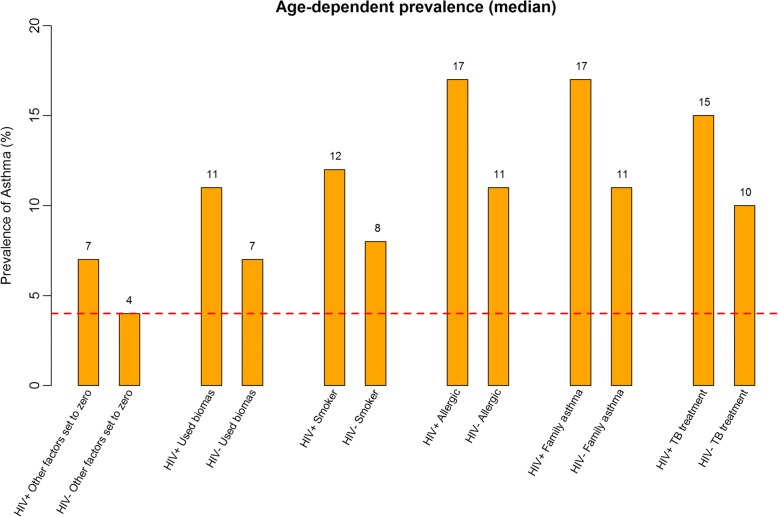
Results: Of 3416 participants, 2067 (60.5%) knew their HIV status and 103 (5.0%) were PLHIV. Asthma prevalence was 15.5% among PLHIV and 9.1% among those without HIV, PR 1.72, (95%CI 1.07-2.75, p = 0.025). HIV modified the association of asthma with the following factors, PLHIV vs. not PLHIV: tobacco smoking (12% vs. 8%, p = < 0.001), biomass use (11% vs. 7%, p = < 0.001), allergy (17% vs. 11%, p = < 0.001), family history of asthma (17% vs. 11%, p = < 0.001), and prior TB treatment (15% vs. 10%, p = < 0.001).
Conclusion: In Uganda the prevalence of asthma is higher in PLHIV than in those without HIV, and HIV interacts synergistically with other known asthma risk factors. Additional studies should explore the mechanisms underlying these associations. Clinicians should consider asthma as a possible diagnosis in PLHIV presenting with respiratory symptoms.
Keywords: Asthma; HIV; Prevalence; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approval was obtained from the Mulago Hospital Research and Ethics committee and the Uganda National Council for Science and Technology. Participants provided written informed consent and were free to terminate study participation at any time during the study. For children between the ages of 12–18 years, we obtained their assent and parental/legal guardian consent.
Consent for publication
Not applicable, this manuscript does not contain any personal data.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Prevalence and factors associated with asthma among adolescents and adults in Uganda: a general population based survey.BMC Public Health. 2019 Feb 22;19(1):227. doi: 10.1186/s12889-019-6562-2. BMC Public Health. 2019. PMID: 30795752 Free PMC article.
-
Reaching the 'first 90': Gaps in coverage of HIV testing among people living with HIV in 16 African countries.PLoS One. 2017 Oct 12;12(10):e0186316. doi: 10.1371/journal.pone.0186316. eCollection 2017. PLoS One. 2017. PMID: 29023510 Free PMC article.
-
People living with HIV travel farther to access healthcare: a population-based geographic analysis from rural Uganda.J Int AIDS Soc. 2016 Feb 10;19(1):20171. doi: 10.7448/IAS.19.1.20171. eCollection 2016. J Int AIDS Soc. 2016. PMID: 26869359 Free PMC article.
-
Depression, suicidality, substance-use and associated factors among people living with HIV the COVID-19 pandemic in Uganda.PLoS One. 2023 May 5;18(5):e0285310. doi: 10.1371/journal.pone.0285310. eCollection 2023. PLoS One. 2023. PMID: 37146057 Free PMC article.
-
Problems of measuring asthma prevalence.Respirology. 1996 Sep;1(3):183-8. doi: 10.1111/j.1440-1843.1996.tb00030.x. Respirology. 1996. PMID: 9424394 Review.
Cited by
-
Health conditions in adults with HIV compared with the general population: A population-based cross-sectional analysis.EClinicalMedicine. 2022 Apr 21;47:101392. doi: 10.1016/j.eclinm.2022.101392. eCollection 2022 May. EClinicalMedicine. 2022. PMID: 35497059 Free PMC article.
-
Effect of HIV on respiratory symptoms, health status, and exertional capacity.AIDS. 2025 Jul 15;39(9):1235-1245. doi: 10.1097/QAD.0000000000004179. Epub 2025 Mar 12. AIDS. 2025. PMID: 40080108
-
Re-estimation of the burden of serious fungal diseases in Uganda.Ther Adv Infect Dis. 2024 Feb 6;11:20499361241228345. doi: 10.1177/20499361241228345. eCollection 2024 Jan-Dec. Ther Adv Infect Dis. 2024. PMID: 38328511 Free PMC article.
-
A Descriptive Analysis of Nasal Polyposis in HIV Positive Versus HIV Negative Patients.Indian J Otolaryngol Head Neck Surg. 2024 Aug;76(4):3289-3297. doi: 10.1007/s12070-024-04674-z. Epub 2024 Apr 10. Indian J Otolaryngol Head Neck Surg. 2024. PMID: 39130228 Free PMC article.
-
Allergy as a Disease of Dysbiosis: Is It Time to Shift the Treatment Paradigm?Front Cell Infect Microbiol. 2019 Mar 7;9:50. doi: 10.3389/fcimb.2019.00050. eCollection 2019. Front Cell Infect Microbiol. 2019. PMID: 30899699 Free PMC article. Review. No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
