

Total Medicare Costs Associated With Diagnosis and Treatment of Prostate Cancer in Elderly Men
- PMID: 30242397
- PMCID: PMC6439776
- DOI: 10.1001/jamaoncol.2018.3701
Total Medicare Costs Associated With Diagnosis and Treatment of Prostate Cancer in Elderly Men
Abstract
Importance: Localized prostate cancer diagnosis and treatment among elderly men who are not likely to benefit represents a potential source of low-value health care services.
Objective: To quantify the costs to the Medicare program associated with detection and treatment of prostate cancer among elderly men in the United States.
Design, setting, and participants: This nationwide, population-based, retrospective cohort study uses the Surveillance, Epidemiology, and End Results (SEER)-Medicare linked database to identify men 70 years or older diagnosed with localized prostate cancer between 2004 and 2007 and to ascertain Medicare costs associated with diagnosis and workup, treatment, follow-up, and morbidity management of the disease. National Medicare costs were estimated using per-person costs, stage-adjusted prostate cancer incidence rates by age from SEER 2007 through 2011, and 2010 Census population estimates by age.
Main outcomes and measures: Estimated costs to the Medicare program overall, and in each (mutually exclusive) category related to diagnosis and workup, treatment, follow-up, and morbidity management.
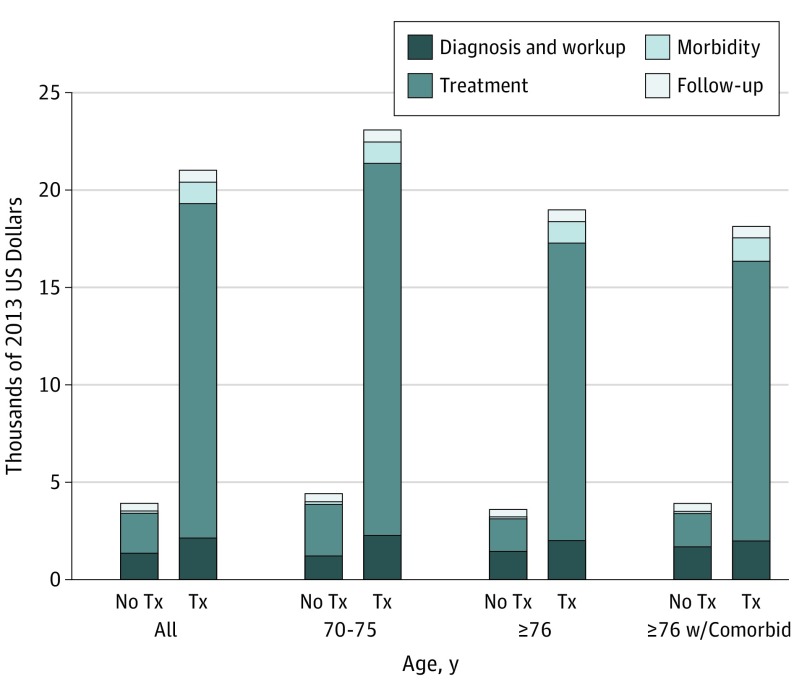
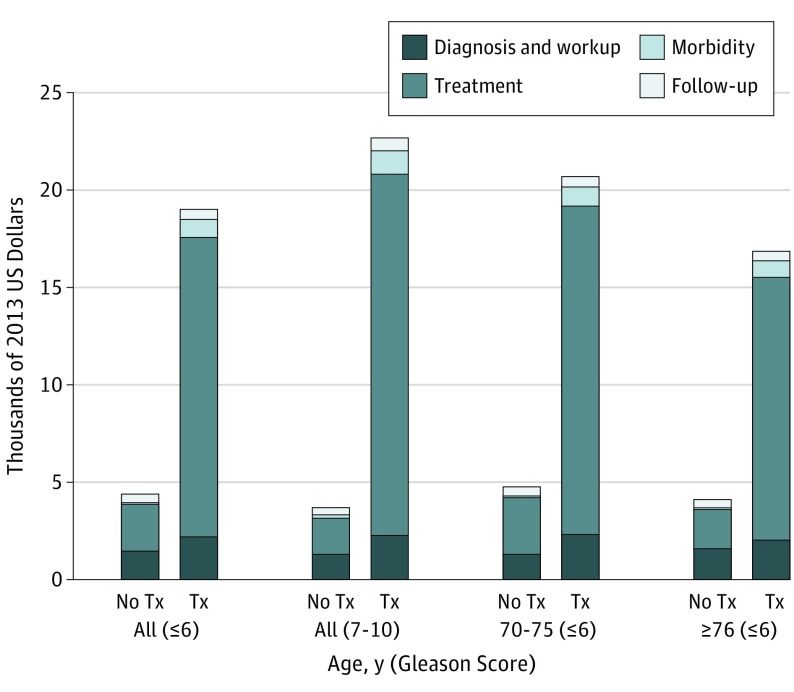
Results: This nationwide, population-based, retrospective cohort study included 49 692 men with nonmetastatic prostate cancer from the SEER-Medicare database (all participants were 70 years or older; 25 981 [52.3%] were 76 years or older). The median per-patient cost within 3 years after prostate cancer diagnosis was $14 453 (interquartile range [IQR], $4887-$27 899). The majority of this cost was attributable to treatment costs (median, $10 558; IQR, $1990-$23 718). Patients with a Gleason score of 6 or lower who pursued initial conservative management (no treatment within 12 months of diagnosis) had a 3-year median total cost of $1914 per patient. The estimated total 3-year cost to the Medicare program associated with the annual detection of prostate cancer in men 70 years or older is approximately $1.2 billion. Increasing active surveillance use in those with Gleason score of 6 or lower could reduce this cost by $320 million.
Conclusions and relevance: There is substantial cost to the Medicare program associated with the diagnosis and treatment of localized prostate cancer among elderly men in the United States, despite the fact that these men are unlikely to die of prostate cancer. The majority of costs are related to treatment. Reducing provision of low-value health care services among this patient population could result in significant health care savings.
Conflict of interest statement
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
