

Optimizing cancer pain management in resource-limited settings
- PMID: 30242544
- PMCID: PMC6499735
- DOI: 10.1007/s00520-018-4471-z
Optimizing cancer pain management in resource-limited settings
Abstract
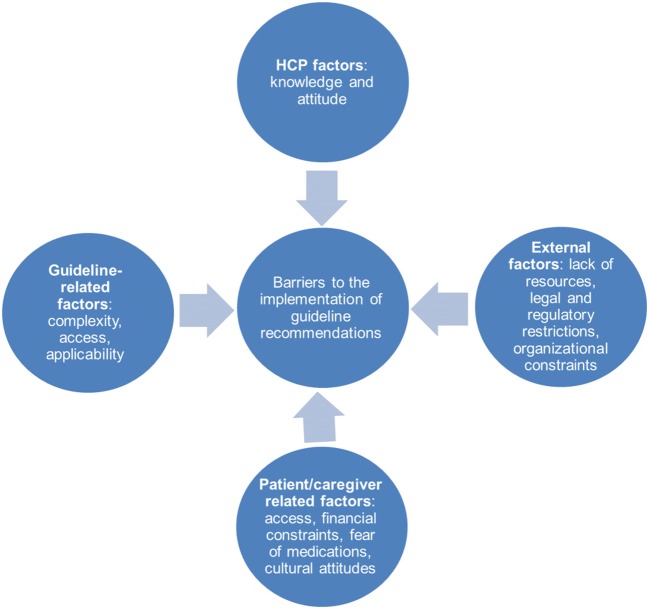
Purpose: Adequate cancer pain management (CPM) is challenging in resource-limited settings, where current international guideline recommendations are difficult to implement owing to constraints such as inadequate availability and accessibility of opioids, limited awareness of appropriate opioid use among patients and clinicians, and lack of guidance on how to translate the best evidence into clinical practice. The multinational and multidisciplinary CAncer Pain managEment in Resource-limited settings (CAPER) Working Group proposes a two-step initiative to bridge clinical practice gaps in CPM in resource-limited settings.
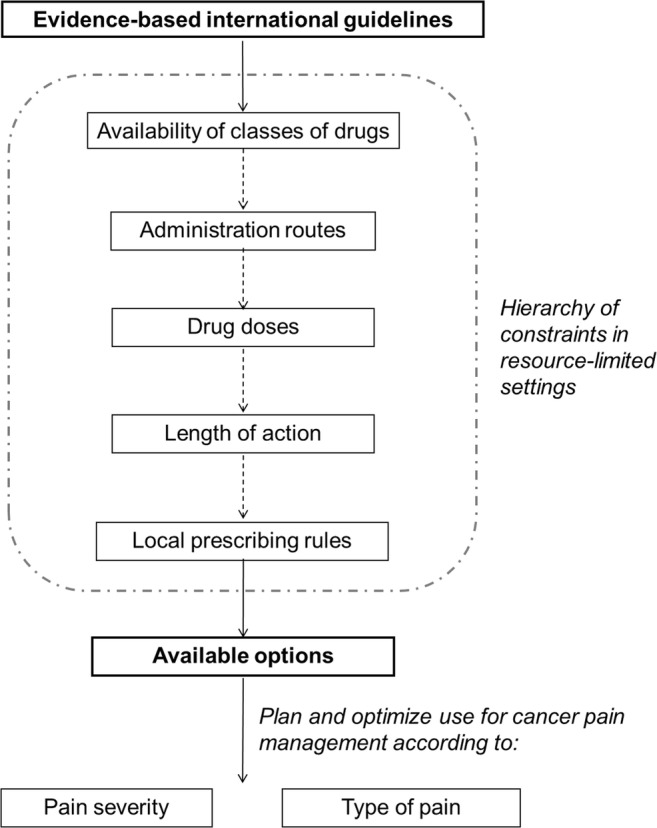
Methods: A thorough review of the literature, a steering committee meeting in February 2017, and post-meeting teleconference discussions contributed to the development of this initiative. As a first step, we developed practical evidence-based CPM algorithms to support healthcare providers (HCPs) in tailoring treatment according to availability of and access to resources. The second part of the initiative proposes a framework to support an effective implementation of the CPM algorithms that includes an educational program, a pilot implementation, and an advocacy plan.
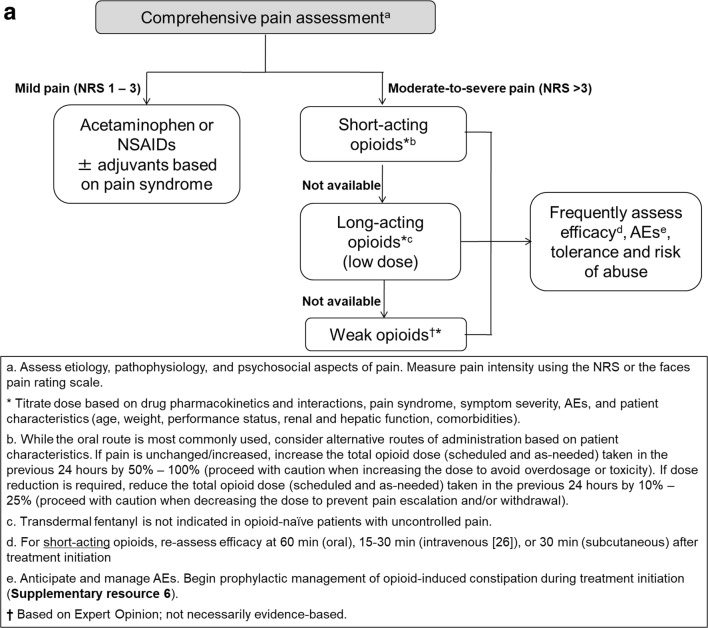
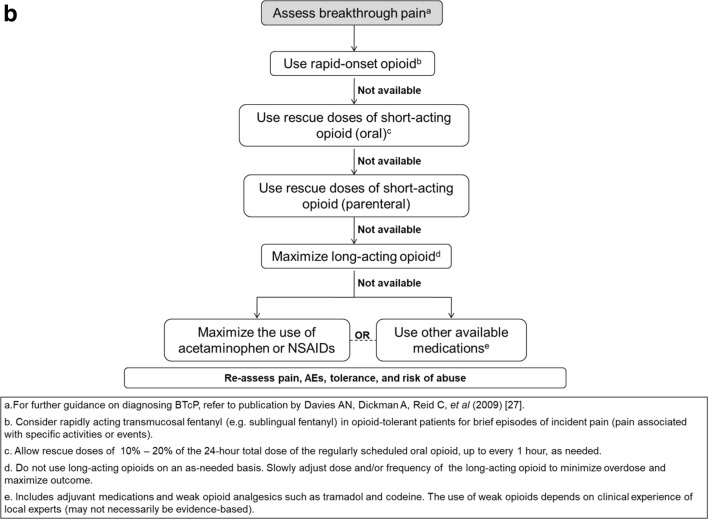
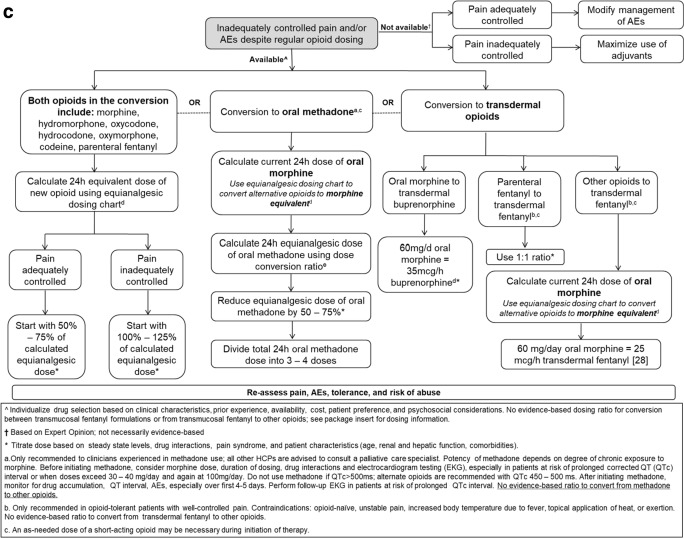
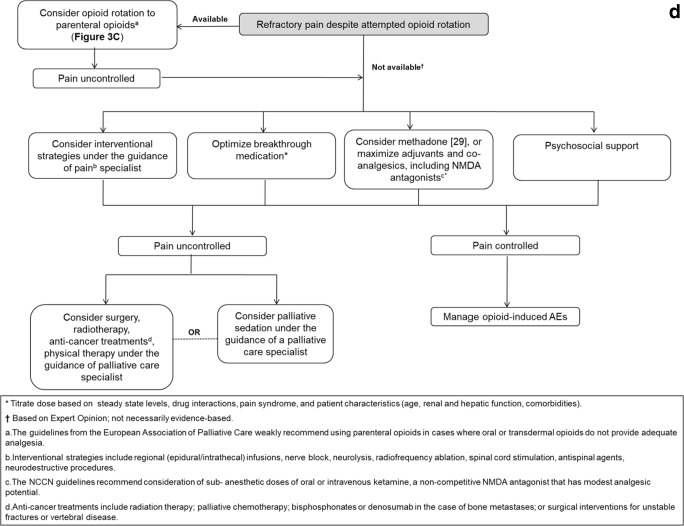
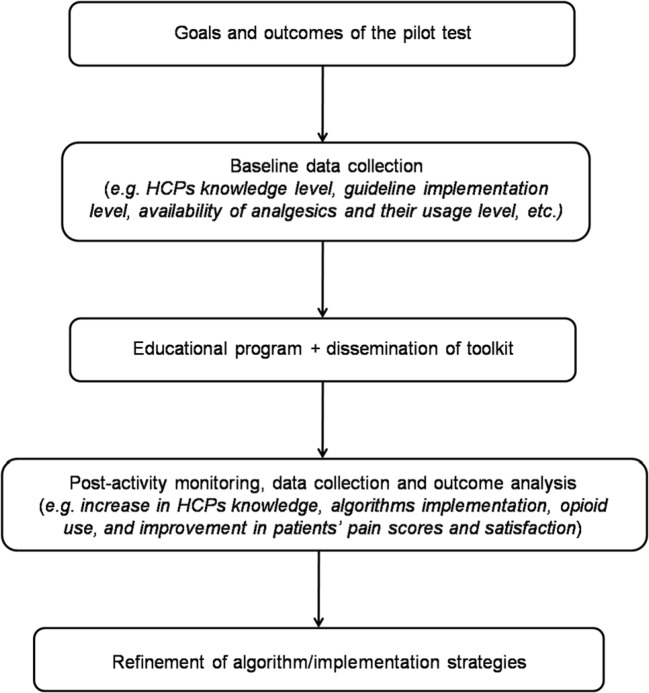
Results: We developed CPM algorithms for first-line use, breakthrough cancer pain, opioid rotation, and refractory cancer pain based on the National Comprehensive Cancer Network guidelines and expert consensus. Our proposed educational program emphasizes the practical elements and illustrates how HCPs can provide optimal CPM according to evidence-based guidelines despite varied resource limitations. Pilot studies are proposed to demonstrate the effectiveness of the algorithms and the educational program, as well as for providing evidence to support a draft advocacy document, to lobby policymakers to improve availability and accessibility of analgesics in resource-limited settings.
Conclusions: These practical evidence-informed algorithms and the implementation framework represent the first multinational step towards achieving optimal CPM in resource-limited settings.
Keywords: Algorithm; Analgesic; Cancer pain; Education; Implementation; Resource-limited.
Conflict of interest statement
MJB, YG, AAIH, SH, DK, DCK, DHL, and JJW received sponsorship from Mundipharma for attending the steering committee meeting.
SHA has received payments for conducting research, giving educational lectures, and taking part in advisory boards with Astra Zeneca, Grünenthal, Mundipharma, and Pfizer; for conducting research with Kyowa Kirin; and for giving educational lectures for Menarini. MJB has received remunerations for lectures given for Johnson and Johnson (formerly Janssen Pharmaceuticals) and Fondazione Menarini. RG has received payments for conducting research, giving educational lectures, and taking part in advisory boards with Onyx, Kaleido Biosciences, and Mundipharma. SH has received lecture fees for Shionogi Pharmaceuticals Co., Mundipharma Japan Co., Taiho Pharmaceutical Co., Daiichi Sankyo Co., Hisamitsu Co., and Teikoku Pharmaceutical Co. DK serves on the Advisory Board of Entrinsic Health Solutions. DCK serves on the Latin America Board of the Grünenthal Group and received remunerations for lectures for Cristalia Produtos Químicos e Farmacêuticos. DHL has received honoraria from AstraZeneca, Boehringer-Ingelheim, Bristol-Myers Squibb, CJ Healthcare, Eli Lilly, Janssen, Merck, MSD, Mundipharma, Novartis, Ono, Pfizer, Roche, Samyang Biopharm, ST Cube, AbbVie, and Takeda for participating in advisory boards. KT has received remunerations for lectures from Kyowa Hakko Kirin Co. Ltd., Ono Pharmaceutical Co., and Eisai Co. JJW has received remunerations for lectures from Eli Lilly, Roche, and Mundipharma. KB, YG, and AAIH have no other conflicts of interest to declare.
Figures
References
-
- van den Beuken-van Everdingen MH, Hochstenbach LM, Joosten EA et al (2016) Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manag 51:1070–1090 - PubMed
-
- Van Riet Paap J, Vissers K, Iliffe S, Radbruch L, Hjermstad MJ, Chattat R, Vernooij-Dassen M, Engels Y, research team IMPACT. Strategies to implement evidence into practice to improve palliative care: recommendations of a nominal group approach with expert opinion leaders. BMC Palliat Care. 2015;14:47. doi: 10.1186/s12904-015-0044-9. - DOI - PMC - PubMed
-
- World Health Organization and Worldwide Palliative Care Alliance (2014) Global atlas of palliative care at the end of life. http://www.who.int/nmh/Global_Atlas_of_Palliative_Care.pdf. Accessed 6 N...
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
