

Impact of oversedation prevention in ventilated critically ill patients: a randomized trial-the AWARE study
- PMID: 30242747
- PMCID: PMC6150862
- DOI: 10.1186/s13613-018-0425-3
Impact of oversedation prevention in ventilated critically ill patients: a randomized trial-the AWARE study
Abstract
Background: Although oversedation has been associated with increased morbidity in ventilated critically ill patients, it is unclear whether prevention of oversedation improves mortality. We aimed to assess 90-day mortality in patients receiving a bundle of interventions to prevent oversedation as compared to usual care.
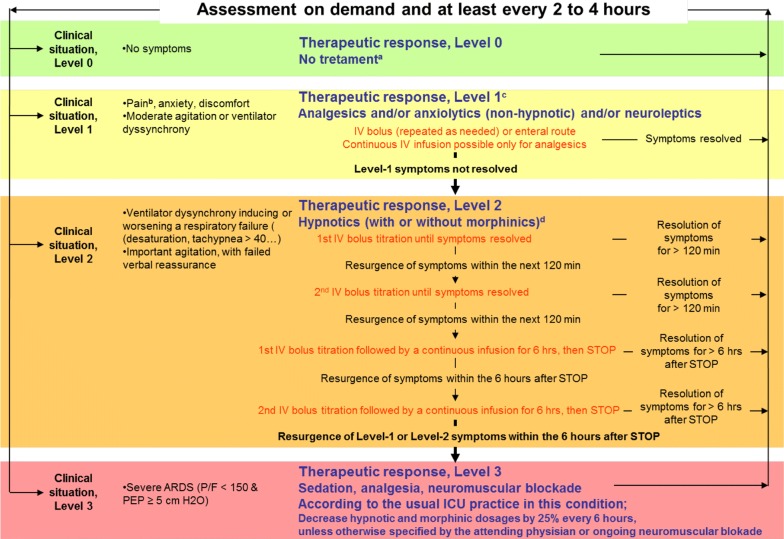
Methods: In this randomized multicentre trial, all adult patients requiring mechanical ventilation for more than 48 h were included. Two groups were compared: patients managed according to usual sedation practices (control), and patients receiving sedation according to an algorithm which provided a gradual multilevel response to pain, agitation, and ventilator dyssynchrony with no specific target to alter consciousness and no use of sedation scale and promoted the use of alternatives to continuous infusion of midazolam or propofol (intervention).
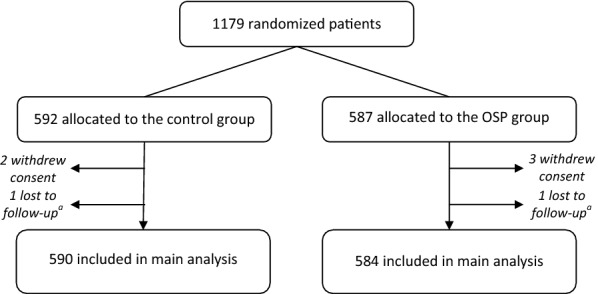
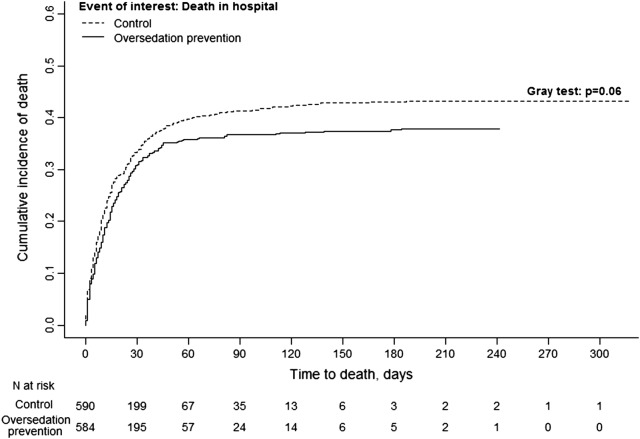
Results: Inclusions were stopped before reaching the planned enrolment. Between 2012 and 2014, 584 patients were included in the intervention group and 590 in the control group. Baseline characteristics were well balanced between groups. Although the use of midazolam and propofol was significantly lower in the intervention group, 90-day mortality was not significantly lower (39.4 vs. 44.2% in the control group, p = 0.09). There were no significant differences in 1-year mortality between the two groups. The time to first spontaneous breathing trial and time to successful extubation were significantly shorter in the intervention group than in the control group. These last results should be interpreted with precaution regarding the several limitations of the trial including the early termination.
Conclusions: This underpowered study of severely ill patients was unable to show that a strategy to prevent oversedation could significantly reduce mortality. Trial registration NCT01617265.
Keywords: Intensive care units; Mechanical ventilation; Mortality; Sedation; Weaning.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
