

Risk factors and outcomes for airway failure versus non-airway failure in the intensive care unit: a multicenter observational study of 1514 extubation procedures
- PMID: 30243304
- PMCID: PMC6151191
- DOI: 10.1186/s13054-018-2150-6
Risk factors and outcomes for airway failure versus non-airway failure in the intensive care unit: a multicenter observational study of 1514 extubation procedures
Abstract
Background: Patients liberated from invasive mechanical ventilation are at risk of extubation failure, including inability to breathe without a tracheal tube (airway failure) or without mechanical ventilation (non-airway failure). We sought to identify respective risk factors for airway failure and non-airway failure following extubation.
Methods: The primary endpoint of this prospective, observational, multicenter study in 26 intensive care units was extubation failure, defined as need for reintubation within 48 h following extubation. A multinomial logistic regression model was used to identify risk factors for airway failure and non-airway failure.
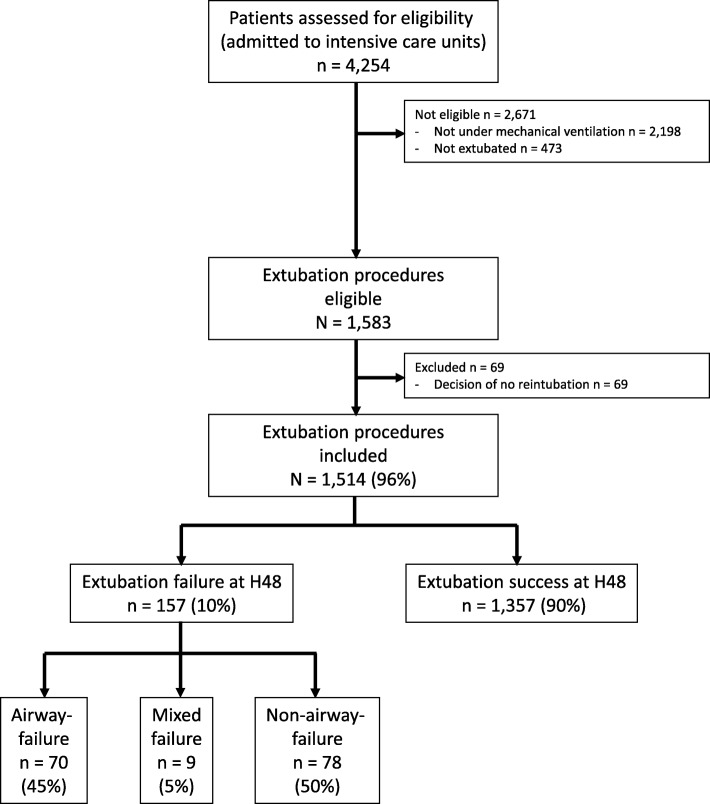
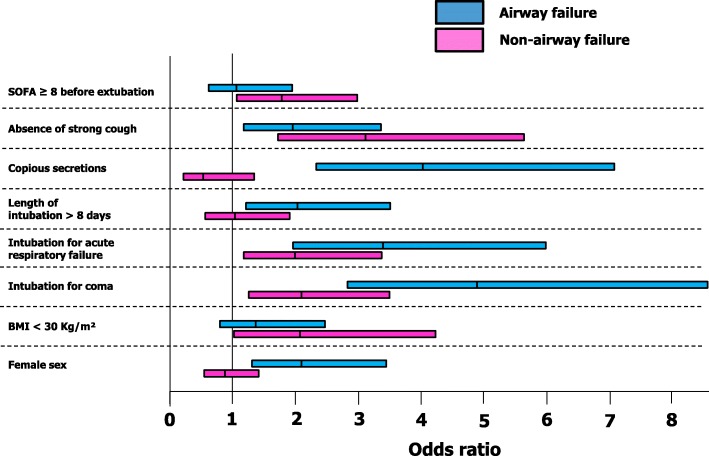
Results: Between 1 December 2013 and 1 May 2015, 1514 patients undergoing extubation were enrolled. The extubation-failure rate was 10.4% (157/1514), including 70/157 (45%) airway failures, 78/157 (50%) non-airway failures, and 9/157 (5%) mixed airway and non-airway failures. By multivariable analysis, risk factors for extubation failure were either common to airway failure and non-airway failure: intubation for coma (OR 4.979 (2.797-8.864), P < 0.0001 and OR 2.067 (1.217-3.510), P = 0.003, respectively, intubation for acute respiratory failure (OR 3.395 (1.877-6.138), P < 0.0001 and OR 2.067 (1.217-3.510), P = 0.007, respectively, absence of strong cough (OR 1.876 (1.047-3.362), P = 0.03 and OR 3.240 (1.786-5.879), P = 0.0001, respectively, or specific to each specific mechanism: female gender (OR 2.024 (1.187-3.450), P = 0.01), length of ventilation > 8 days (OR 1.956 (1.087-3.518), P = 0.025), copious secretions (OR 4.066 (2.268-7.292), P < 0.0001) were specific to airway failure, whereas non-obese status (OR 2.153 (1.052-4.408), P = 0.036) and sequential organ failure assessment (SOFA) score ≥ 8 (OR 1.848 (1.100-3.105), P = 0.02) were specific to non-airway failure. Both airway failure and non-airway failure were associated with ICU mortality (20% and 22%, respectively, as compared to 6% in patients with extubation success, P < 0.0001).
Conclusions: Specific risk factors have been identified, allowing us to distinguish between risk of airway failure and non-airway failure. The two conditions will be managed differently, both for prevention and curative strategies.
Trial registration: ClinicalTrials.gov, NCT 02450669 . Registered on 21 May 2015.
Trial registration: ClinicalTrials.gov NCT02450669.
Keywords: Airway; Extubation; Non-airway, weaning.
Conflict of interest statement
Ethics approval and consent to participate
The appropriate IRB (
Consent for publication
Not applicable.
Competing interests
Pr Jaber reports receiving consulting fees from Drager, Hamilton, Maquet and Fisher & Paykel.
Elie Azoulay has received fees from Gilead Sciences, Alexion, Astellas, MSD and Drager.
Julien Pottecher has received fees from Medtronic, Baxter and Getinge. The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Jaber S, Bellani G, Blanch L, Demoule A, Esteban A, Gattinoni L, Guérin C, Hill N, Laffey JG, Maggiore SM, et al. The intensive care medicine research agenda for airways, invasive and noninvasive mechanical ventilation. Intensive Care Med. 2017;43(9):1352–1365. doi: 10.1007/s00134-017-4896-8. - DOI - PubMed
-
- Asehnoune K, Mrozek S, Perrigault PF, Seguin P, Dahyot-Fizelier C, Lasocki S, Pujol A, Martin M, Chabanne R, Muller L, et al. A multi-faceted strategy to reduce ventilation-associated mortality in brain-injured patients. The BI-VILI project: a nationwide quality improvement project. Intensive Care Med. 2017;43(7):957–970. doi: 10.1007/s00134-017-4764-6. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
