

Impact of left atrial compliance improvement on functional status after percutaneous mitral valvuloplasty
- PMID: 30244517
- PMCID: PMC8272835
- DOI: 10.1002/ccd.27831
Impact of left atrial compliance improvement on functional status after percutaneous mitral valvuloplasty
Abstract
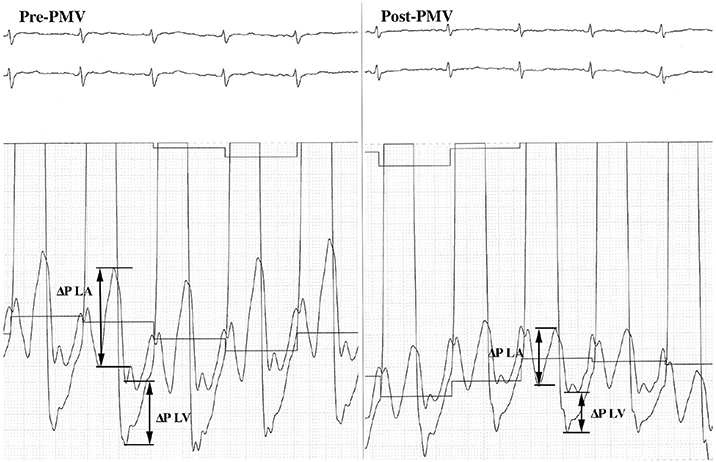
Background: Conventional hemodynamic parameters may not accurately predict symptomatic improvement after percutaneous mitral valvuloplasty (PMV). Changes in left heart chamber compliance following adequate relief o0066 mitral stenosis (MS) may be useful in determining functional capacity after PMV. This study aims to determine the acute effects of PMV on compliance of the left heart and whether its changes relate to the patient's functional capacity.
Methods: One-hundred thirty-seven patients with severe MS undergoing PMV were enrolled. Left atrial (Ca ) and left ventricular (Cv ) compliance were invasively estimated and net atrioventricular compliance (Cav ) was calculated before and immediately after the procedure. B-type natriuretic peptide (BNP) levels were obtained before and 24 hr after the procedure. The primary endpoint was functional status at 6-month follow-up, and the secondary endpoint was a composite of death, mitral valve (MV) replacement, repeat PMV, new onset of atrial fibrillation, or stroke in patients in whom PMV was successful.
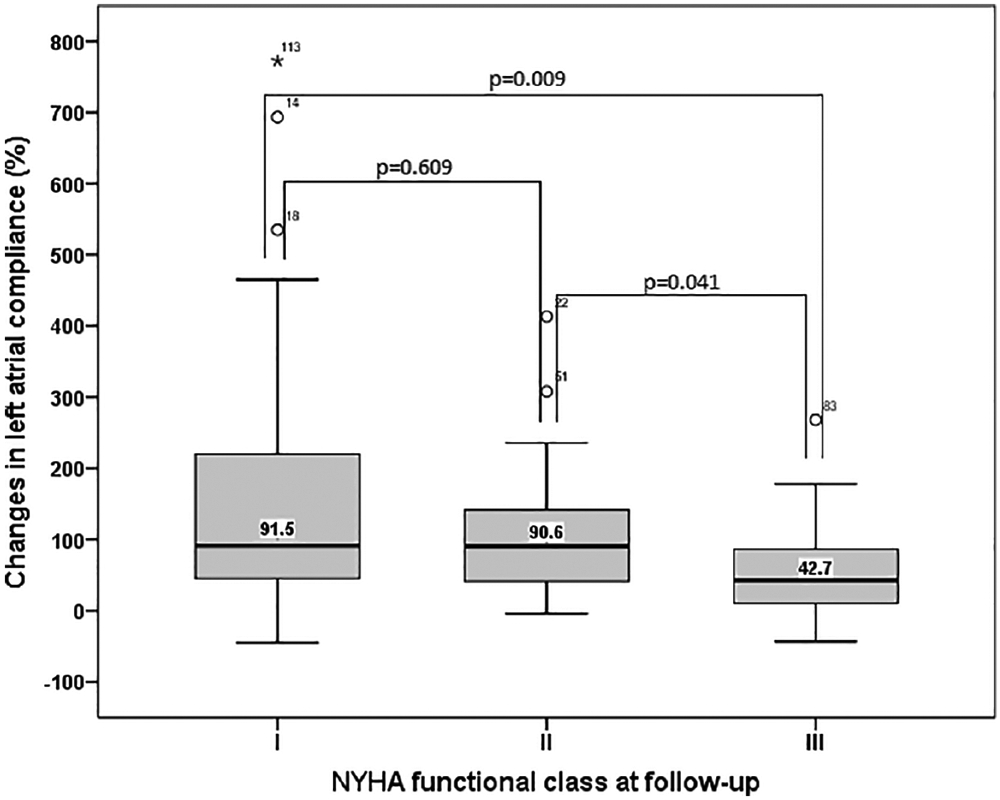
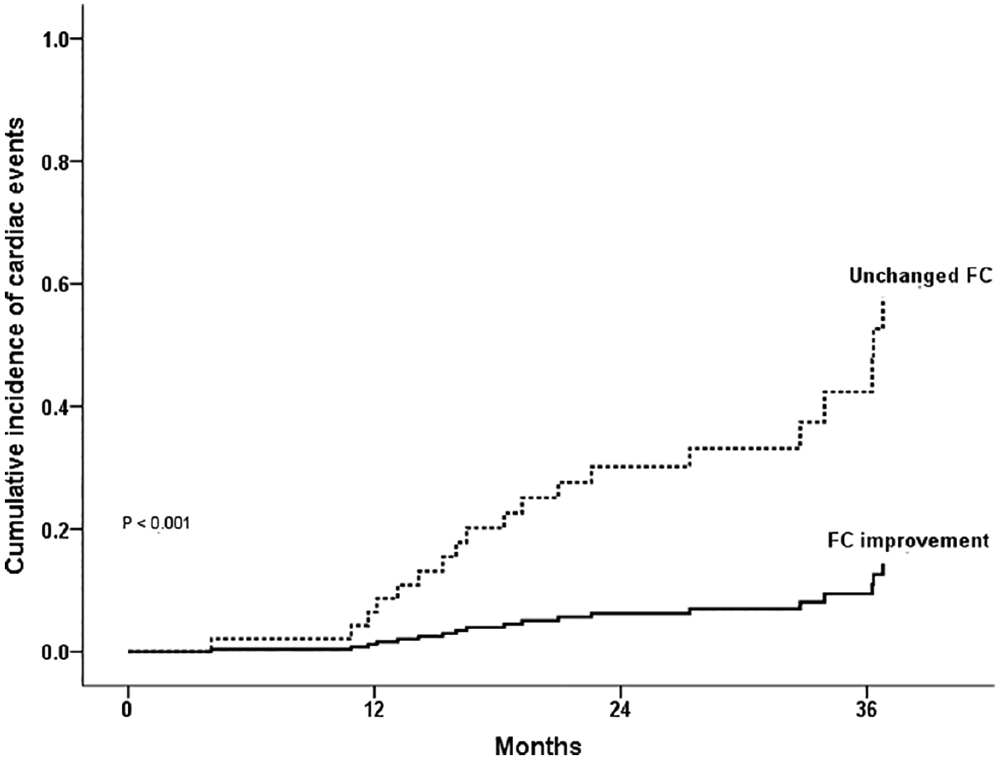
Results: The mean age was 43 ± 12 years, and 119 patients were female (87%). After PMV, Ca and Cav improved significantly from 5.3 [IQR 3.2-8.2] mL/mmHg to 8.7 [5.3-19.2] mL/mmHg (P < 0.001) and 2.2 [1.6-3.4] to 2.8 [2.1-4.1] mL/mmHg (P < 0.001), respectively, whereas Cv did not change (4.6 [3.2-6.8] to 4.4 [3.1-5.6]; P = 0.637). Plasma BNP levels significantly decreased after PMV, with no correlation between its variation and changes in left chamber compliance. At 6-month follow-up, NYHA functional class remained unchanged in 32 patients (23%). By multivariable analyses, changes in Ca immediately after PMV (adjusted OR 1.42; 95% CI 95% 1.02 to 1.97; P = 0.037) and younger age (adjusted OR 0.95; CI 95% 0.92-0.98; P = 0.004), predicted improvement in functional capacity at 6-month follow-up, independent of postprocedural data. The secondary endpoint were predicted by post-PMV mean gradient (adjusted HR 1.363; 95% CI 95% 1.027-1.809; P = 0.032), and lack of functional improvement at 6-month follow-up (adjusted HR 4.959; 95% 1.708-14.403; P = 0.003).
Conclusions: Ca and Cav increase significantly after PMV with no change in Cv . The improvement of Ca is an important predictor of functional status at 6-month follow up, independently of other hemodynamic data. Postprocedural mean gradient and lack of short-term symptomatic improvement were predictors of adverse outcome.
Keywords: atrial compliance; functional capacity; mitral stenosis; net atrioventricular compliance; percutaneous mitral valvuloplasy; ventricular compliance.
© 2018 Wiley Periodicals, Inc.
Figures
Similar articles
-
Net atrioventricular compliance is an independent predictor of cardiovascular death in mitral stenosis.Heart. 2017 Dec;103(23):1891-1898. doi: 10.1136/heartjnl-2016-310955. Epub 2017 Aug 5. Heart. 2017. PMID: 28780580
-
Pulmonary artery pressure response to percutaneous mitral valvuloplasty: Associated factors and clinical implications.Catheter Cardiovasc Interv. 2022 Feb;99(3):915-923. doi: 10.1002/ccd.29926. Epub 2021 Aug 20. Catheter Cardiovasc Interv. 2022. PMID: 34415669
-
Impact of percutaneous mitral valvuloplasty on left ventricular function in patients with mitral stenosis assessed by 3D echocardiography.Int J Cardiol. 2017 Dec 1;248:280-285. doi: 10.1016/j.ijcard.2017.06.078. Epub 2017 Jun 23. Int J Cardiol. 2017. PMID: 28712559
-
Advances in Rheumatic Mitral Stenosis: Echocardiographic, Pathophysiologic, and Hemodynamic Considerations.J Am Soc Echocardiogr. 2021 Jul;34(7):709-722.e1. doi: 10.1016/j.echo.2021.02.015. Epub 2021 Feb 27. J Am Soc Echocardiogr. 2021. PMID: 33652082 Review.
-
[Immediate results and mid-term follow-up after percutaneous mitral valve replacement].Arch Mal Coeur Vaiss. 1991 Sep;84(9):1311-9. Arch Mal Coeur Vaiss. 1991. PMID: 1835571 Review. French.
Cited by
-
Cardiovascular Statistics - Brazil 2021.Arq Bras Cardiol. 2022 Jan;118(1):115-373. doi: 10.36660/abc.20211012. Arq Bras Cardiol. 2022. PMID: 35195219 Free PMC article. English, Portuguese. No abstract available.
-
Left atrial function in patients with rheumatic mitral stenosis: addressing prognostic insights beyond atrial fibrillation prediction.Eur Heart J Imaging Methods Pract. 2024 Jul 12;2(2):qyae067. doi: 10.1093/ehjimp/qyae067. eCollection 2024 Apr. Eur Heart J Imaging Methods Pract. 2024. PMID: 39224865 Free PMC article.
-
Augmenting mitral valve repair evaluation with intraoperative left ventricle pressure measurements.Interact Cardiovasc Thorac Surg. 2022 Oct 10;35(5):ivac242. doi: 10.1093/icvts/ivac242. Interact Cardiovasc Thorac Surg. 2022. PMID: 36173329 Free PMC article.
-
Efficacy and safety of percutaneous mitral balloon valvotomy in patients with mitral stenosis: A systematic review and meta-analysis.Int J Cardiol Heart Vasc. 2021 Apr 1;33:100765. doi: 10.1016/j.ijcha.2021.100765. eCollection 2021 Apr. Int J Cardiol Heart Vasc. 2021. PMID: 33889711 Free PMC article.
References
-
- Watkins DA, Johnson CO, Colquhoun SM, et al. Global, regional, and national burden of rheumatic heart disease, 1990-2015. N Engl J Med. 2017;377:713–722. - PubMed
-
- Chandrashekhar Y, Westaby S, Narula J. Mitral stenosis. Lancet. 2009; 374:1271–1283. - PubMed
-
- Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP III, Guyton RA, O'Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM III, Thomas JD, Anderson JL, Halperin JL, Albert NM, Bozkurt B, Brindis RG, Creager MA, Curtis LH, DeMets D, Guyton RA, Hochman JS, Kovacs RJ, Ohman EM, Pressler SJ, Sellke FW, Shen WK, Stevenson WG, Yancy CW; American College of Cardiology; American College of Cardiology/American Heart Association; American Heart Association. 2014 aha/acc guideline for the management of patients with valvular heart disease: A report of the american college of cardiology/American heart association task force on practice guidelines. J Thorac Cardiovasc Surg 2014;148:e1–e132. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
